
Triceps Tendon Rupture
Overview
Triceps tendon rupture is rare — the least common tendon rupture in the upper limb, accounting for <1% of all tendon injuries. The triceps inserts via its tendon onto the olecranon process of the ulna. The most common injury pattern is avulsion of the distal triceps tendon from the olecranon, caused by a direct fall onto the elbow or eccentric contraction (attempted prevention of elbow flexion collapse during weight-bearing). Risk factors include anabolic steroid use, hyperparathyroidism, and systemic lupus erythematosus.
Symptoms & Diagnosis
- Posterior elbow pain and swelling following a fall or resisted extension effort
- Weakness or inability to actively extend the elbow against gravity — the key clinical finding
- Palpable gap in the triceps tendon 1–2 cm proximal to the olecranon
- Modified Thompson squeeze test (forearm): Squeezing the posterior forearm does not produce the expected elbow extension — analogous to Thompson’s test for Achilles rupture
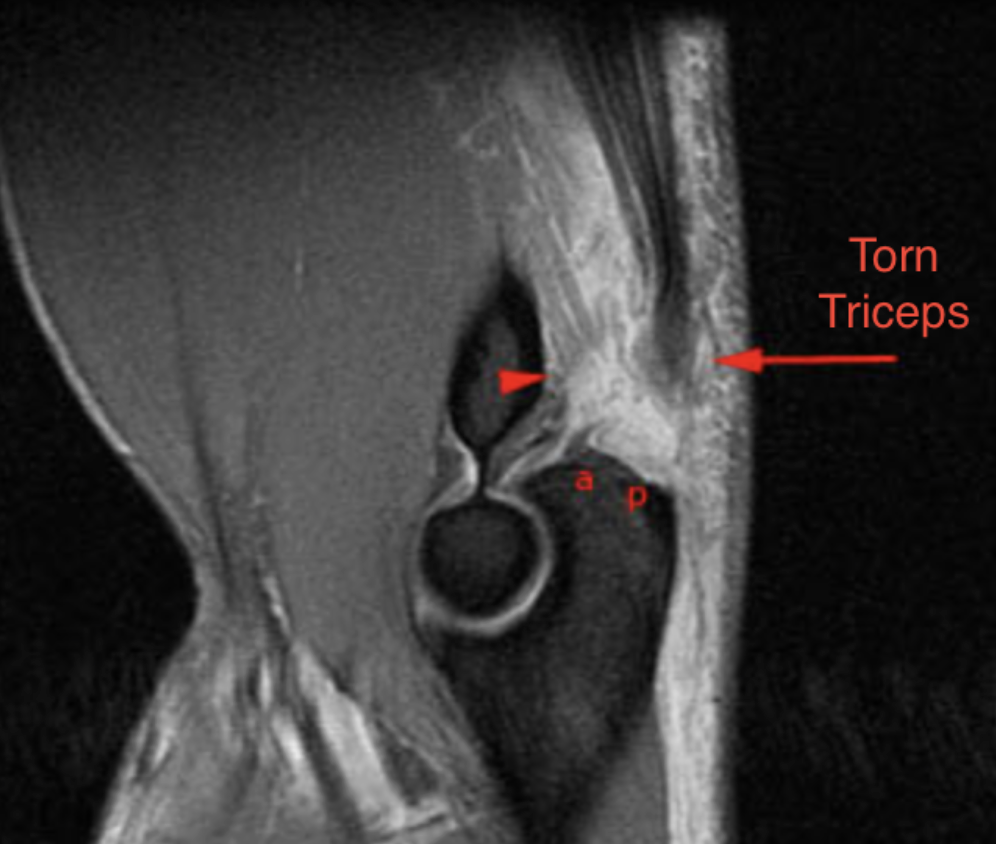
- MRI: Confirmatory — shows the level of disruption, degree of retraction, and whether repair is feasible. Partial tears can be distinguished from complete ruptures.
Treatment
- Complete ruptures in active patients: Surgical repair. The tendon is reattached to the olecranon using transosseous sutures, suture anchors, or a combination. Early repair (<4 weeks) is preferred. Recovery similar to distal biceps repair: 4–6 months to full function.
- Partial tears and older, low-demand patients: Conservative management with splinting in 30–40° elbow flexion for 4–6 weeks, followed by graduated physiotherapy.
Patient FAQs –Triceps Tendon Rupture
I can still extend my elbow slightly — does that mean it isn't ruptured?
Partial triceps tears may preserve some extension power through intact fibres or via the anconeus muscle. However, a palpable gap and pain with resisted extension should prompt urgent MRI. Even apparent partial tears may be complete on imaging. Please seek early assessment.
















