
Lateral Epicondylitis (Tennis Elbow)
Overview & Anatomy
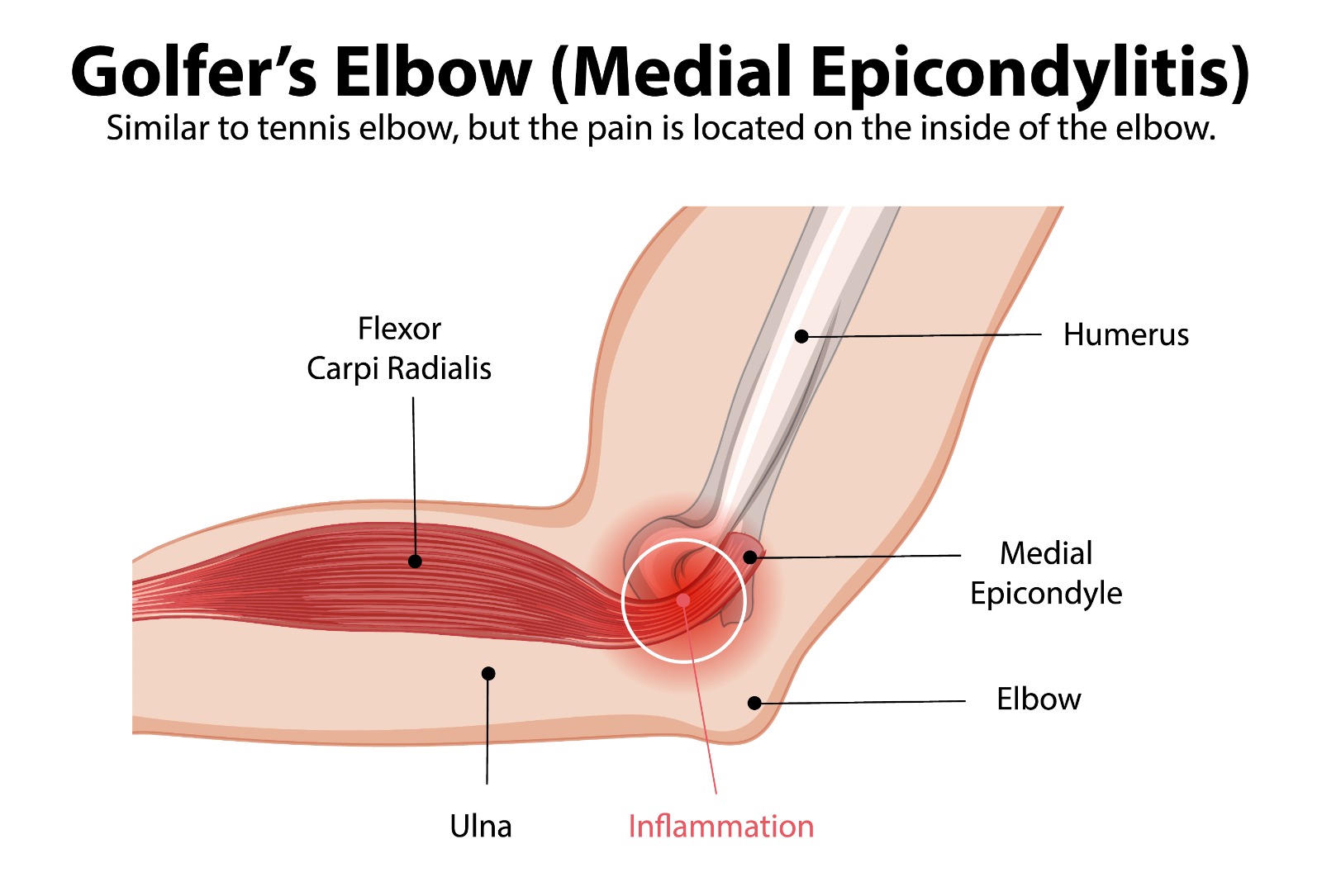
Medial epicondylitis — golfer’s elbow — is a tendinopathy of the common flexor origin at the medial epicondyle of the humerus. It is approximately 4–7 times less common than tennis elbow. The pronator teres and flexor carpi radialis are the most frequently affected tendons. As with lateral epicondylitis, the histological picture is angiofibroblastic tendinosis rather than true inflammation.
The proximity of the ulnar nerve to the medial epicondyle is clinically important — up to 60% of patients with medial epicondylitis have concurrent cubital tunnel syndrome (ulnar nerve irritation), and this dual pathology must be recognised and addressed simultaneously to achieve satisfactory outcomes.
Causes & Risk Factors
- Repetitive valgus loading combined with wrist flexion and forearm pronation
- Occupational: Carpentry, plumbing, heavy tool use, throwing occupations
- Sports: Golf (leading arm at impact), baseball pitching, javelin, tennis (forehand topspin), weightlifting
- Age 35–60; slightly more common in women
Symptoms
- Medial elbow pain with point tenderness 1–2 cm distal to the medial epicondyle over the common flexor origin
- Pain reproduced by resisted wrist flexion and forearm pronation with elbow extended
- Grip weakness — particularly when carrying objects with palm facing down
- Associated ulnar nerve symptoms: Tingling or numbness in the ring and little fingers (cubital tunnel syndrome) — must be specifically asked about and examined
- Pain on the golf downswing and at impact (leading arm in right-handed golfer)
Diagnosis & Treatment
Assessment mirrors that of tennis elbow, with the important addition of ulnar nerve examination. Tinel’s sign over the cubital tunnel and elbow flexion test (sustained elbow flexion >60 seconds reproducing ulnar nerve symptoms) must be performed.
Treatment follows the same pathway as lateral epicondylitis: physiotherapy with progressive flexor-pronator loading exercises is first-line, supported by counterforce bracing, topical NSAIDs, and selective PRP or steroid injection. Where concurrent cubital tunnel syndrome exists, ulnar nerve management is addressed simultaneously — see Chapter 4.
Surgical Treatment

- Medial epicondyle release and debridement: Open or arthroscopic-assisted approach. The degenerative flexor-pronator origin tissue is excised and the healthy tendon edges refreshed. Performed as day surgery.
- Ulnar nerve transposition: If concurrent cubital tunnel syndrome has failed non-surgical management, the ulnar nerve is simultaneously relocated anteriorly during the medial epicondyle procedure, eliminating the need for a second operation.
Patient FAQs – Medial Epicondylitis (Golfer's Elbow)
Can golfer's elbow and tennis elbow occur together?
Yes — though uncommon. Simultaneous medial and lateral epicondylitis occurs in patients with very high elbow loading demands. Each is managed independently. Dr. Senthilvelan will identify and address all sites of pathology.
I have tingling in my ring and little finger as well as elbow pain — is this related?
Very likely, yes. Ulnar nerve irritation at the cubital tunnel is present in up to 60% of medial epicondylitis patients. The two conditions share the same anatomical region and are commonly seen together. Both need to be treated — addressing the tendon alone while leaving the nerve irritated will result in an incomplete response.
















