
Distal Biceps Tendon Rupture
Overview
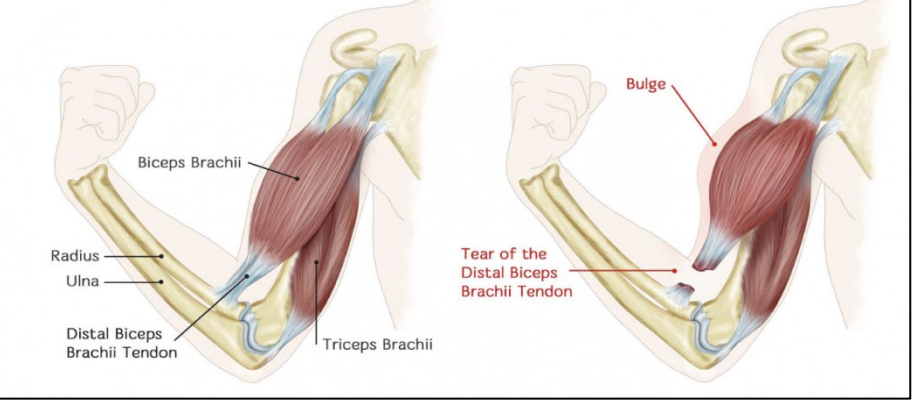
Distal biceps tendon rupture — avulsion of the biceps tendon from its insertion on the radial tuberosity — is a distinct injury from the proximal long head biceps rupture at the shoulder. It accounts for only 3–5% of biceps tendon injuries but has far greater functional consequences: complete distal rupture causes a 40% loss of supination strength and a 30% loss of elbow flexion power — deficits that are clinically significant and persistent without repair.
Mechanism & Presentation
- Mechanism: Sudden eccentric load on a partially flexed, supinated forearm — typically lifting a heavy object that is heavier than anticipated, or catching a falling weight
- Predominantly affects men aged 40–60; associated with anabolic steroid use and smoking (both compromise tendon vascularity)
- Acute presentation: A sharp tearing pain in the antecubital fossa (front of the elbow), immediate bruising and swelling, a palpable gap or abnormal soft tissue contour in the antecubital fossa
- The ‘hook test’: The examiner hooks a finger around the lateral border of the biceps tendon in the antecubital fossa — the tendon cannot be hooked in a complete rupture. Sensitivity >80%, specificity >90%.
- Reverse Popeye sign: Proximal retraction of the biceps muscle belly (opposite to the distal Popeye deformity of proximal rupture)
Diagnosis
- Clinical examination and hook test are usually sufficient for diagnosis in the acute setting
- MRI: Confirms complete vs partial tear, documents retraction distance, and excludes concurrent pathology. Essential if the hook test is equivocal or when partial tear is suspected.
- Ultrasound: Dynamic assessment; experienced hands can reliably diagnose complete distal rupture
Treatment
Key principle: Surgical repair is strongly recommended for all active patients under 70 with complete distal biceps rupture. Functional deficits from non-surgical management are significant and permanent. Outcomes are best when repair is performed within 2–4 weeks of injury — delayed repair requires tendon graft augmentation.
Surgical Repair
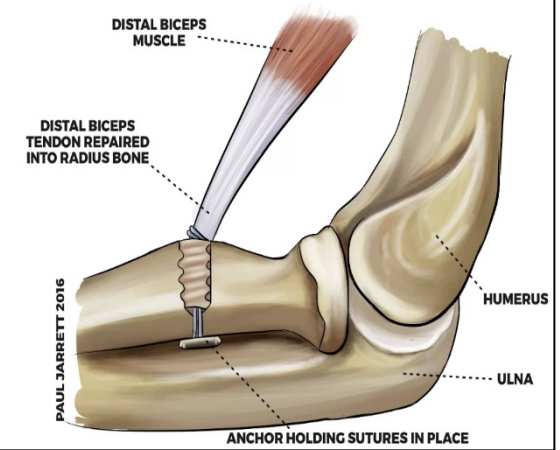
- Single-incision anterior technique (Dr. Senthilvelan’s preferred approach): The tendon is retrieved through a single transverse incision in the antecubital fossa and reattached to the radial tuberosity using cortical button fixation (EndoButton) or suture anchors. Biomechanically superior to older two-incision techniques with lower risk of radioulnar synostosis.
- Two-incision technique (Boyd-Anderson): An anterior incision retrieves the tendon; a posterior incision provides access to the radial tuberosity for bony attachment. Lower risk of heterotopic ossification with modern technique modifications.
- Recovery: Sling for 2 weeks; active flexion-extension from 2 weeks; forearm rotation exercises from 4 weeks; strengthening from 8 weeks; full recovery at 4–6 months.
Non-Surgical (Older Patients, Low Demand)
In patients over 65–70 with low physical demands, non-surgical management is acceptable. Elbow flexion strength is relatively well maintained; supination weakness is the main functional deficit, usually compensated within weeks to months by forearm musculature adaptation.
Patient FAQs –Distal Biceps Tendon Rupture
How urgent is surgery for distal biceps rupture?
Early repair (within 2–4 weeks) is strongly preferred. The tendon retracts proximally with time, and muscle shortening makes direct repair increasingly difficult. After 4–6 weeks, a tendon graft augmentation procedure may be required. If you suspect a distal biceps rupture, contact Dr. Senthilvelan’s clinic urgently for assessment.
Can I lift weights again after distal biceps repair?
Yes — a successful distal biceps repair restores full supination strength and near-full flexion power. Return to gym activities is expected at 4–6 months. High-demand athletes (weightlifters, gymnasts) can typically return to full training at 6 months with appropriate load progression.
















