")
Total Elbow Replacement (Arthroplasty)
Overview
Total elbow replacement (TER) — or total elbow arthroplasty (TEA) — replaces the diseased articular surfaces of the distal humerus and proximal ulna (and radial head when required) with a linked or unlinked prosthetic implant. It is less commonly performed than hip or knee replacement but is a highly effective procedure for appropriately selected patients with end-stage elbow arthritis or complex fractures.
Indications
- Rheumatoid arthritis: The most common indication for TER. RA causes progressive bilateral elbow destruction and TER provides reliable, durable pain relief and functional restoration.
- Osteoarthritis: Reserved for severe end-stage OA where arthroscopic debridement has failed and the patient has insufficient bone stock for simpler procedures
- Post-traumatic arthritis: Following complex elbow fractures, non-unions, or failed prior surgery
- Complex distal humerus fractures in elderly patients: Primary TER avoids the challenges of complex ORIF in osteoporotic bone and allows faster rehabilitation
Implant Types
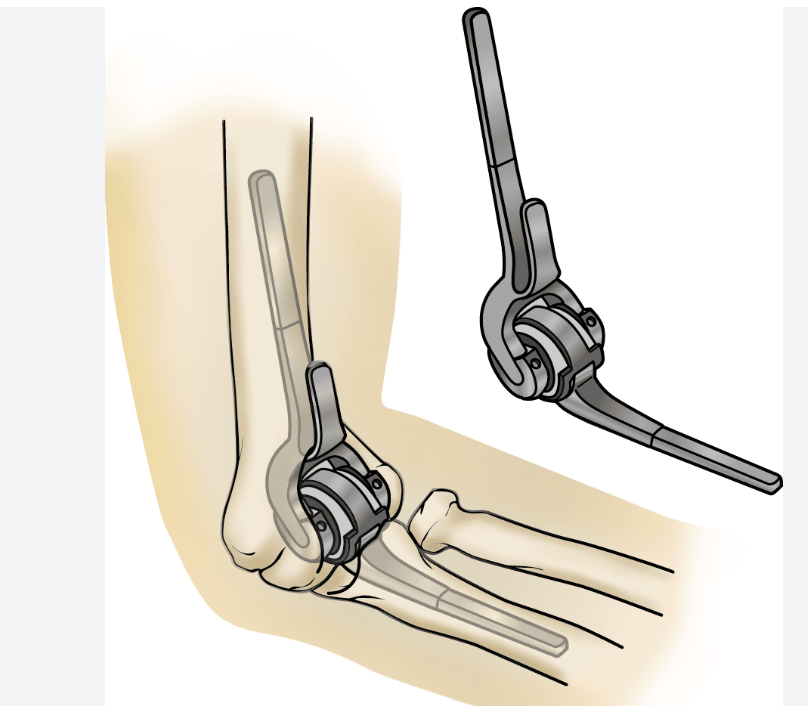
Linked (Semi-Constrained) | The humeral and ulnar components are connected by a pin mechanism with intentional laxity. The most commonly used type. Not reliant on collateral ligament integrity. The Coonrad-Morrey prosthesis is the gold standard linked implant with >20-year follow-up data. |
Unlinked (Unconstrained) | Components are not directly connected — joint stability depends on intact collateral ligaments. Lower constraint means less bone-cement interface stress but requires adequate ligamentous stability. |
The Procedure
Total elbow replacement is performed under general anaesthesia with a tourniquet. A posterior midline incision provides exposure. The triceps mechanism is reflected (or split) to expose the joint; the diseased articular surfaces are resected with precision cuts; and the implants are secured with bone cement. The triceps is meticulously repaired and the wound closed.
Recovery & Rehabilitation
0–6 weeks | Arm in a posterior plaster splint or hinged brace. Wound care, hand and wrist exercises. Elbow motion commences at 1–2 weeks. |
6–12 weeks | Progressive active elbow range of motion. Physiotherapy-supervised strengthening. No load-bearing. |
3–6 months | Full daily activities restored. Light functional use permitted. |
Permanent restriction | Lifetime restriction on lifting >2 kg single arm or >5 kg total. No impact loading. Implant longevity depends on adherence to these restrictions. |
Lifetime weight restriction: All patients with a total elbow replacement must observe a permanent lifting restriction of approximately 1–2 kg in the operated arm for single lifts. This is non-negotiable — excessive loading significantly reduces implant longevity and risks periprosthetic fracture.
Outcomes & Implant Longevity
- Pain relief: Excellent — >90% of patients report significant or complete relief of rest and activity pain
- Range of motion: Mean flexion arc of 25°–130° typically achieved
- Implant survival: 10-year survival approximately 80–90% for rheumatoid arthritis; somewhat lower for post-traumatic cases due to younger, more active patients and higher mechanical demands
- Complications: Infection (2–4%), triceps weakness or detachment, periprosthetic fracture, bushing wear and loosening, and ulnar nerve injury
Patient FAQs –Throwing Elbow & Medial UCL Injury
Will I have full use of my arm after elbow replacement?
You will regain the ability to perform most daily activities — eating, washing, dressing, light computer work, and writing. The permanent weight restriction means heavy lifting, manual labour, and impact sports are not compatible with a long-lived implant. The primary goal is a pain-free, functional arm for everyday life.
How long does a total elbow replacement last?
Published series show 80–90% implant survival at 10 years in rheumatoid patients. Younger, more active patients have higher revision rates. With careful patient selection and strict adherence to activity restrictions, modern TER implants can last 15–20 years.
Can both elbows be replaced?
Yes — in rheumatoid arthritis patients with bilateral elbow destruction, sequential bilateral TER is performed. The dominant arm is usually operated first. Staging the procedures approximately 3–6 months apart allows optimal rehabilitation of each arm.
















