
Olecranon Bursitis
Overview
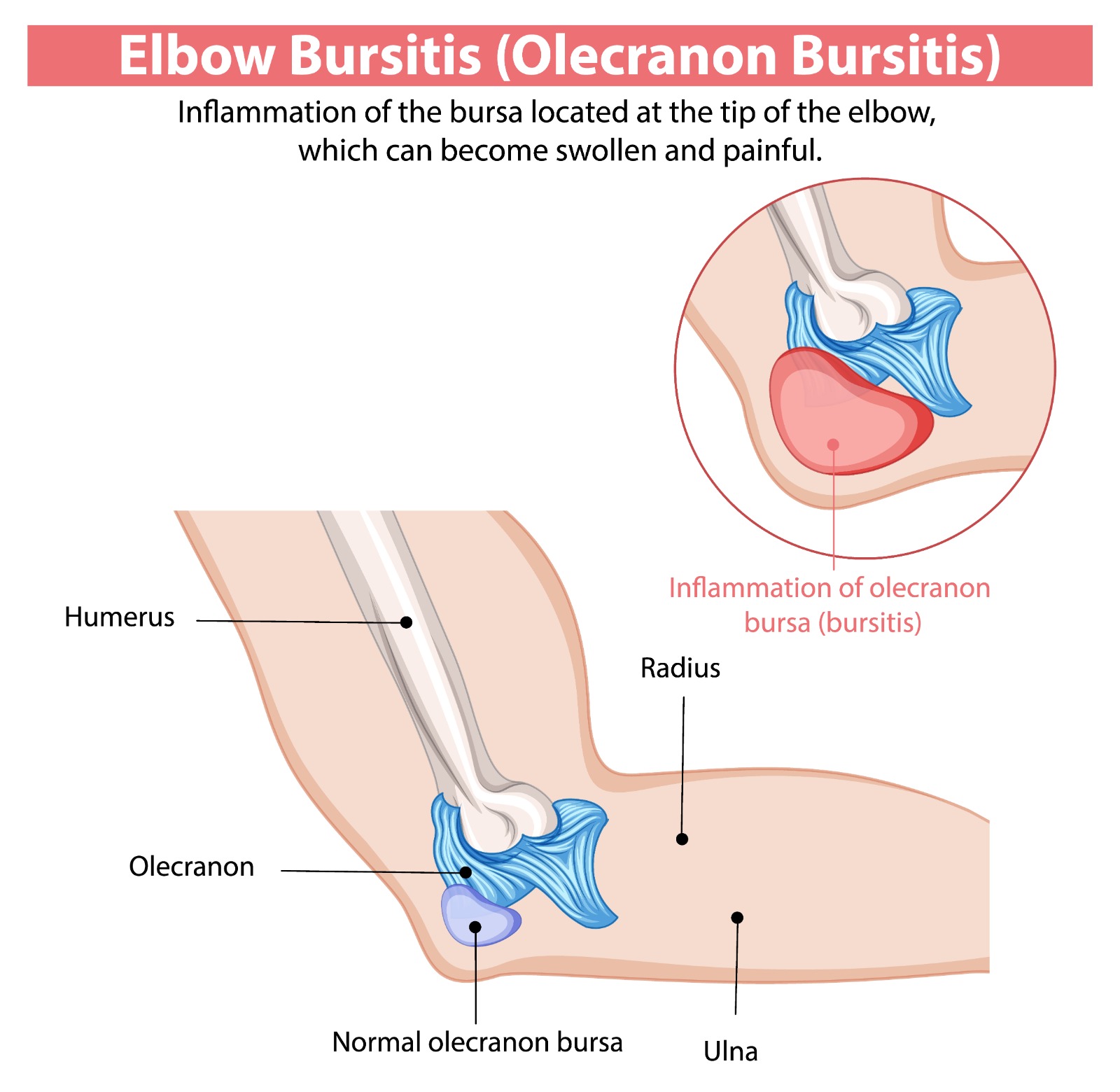
Olecranon bursitis is inflammation and fluid accumulation in the olecranon bursa — a small synovial sac overlying the olecranon process at the tip of the elbow. It is one of the most common bursitis conditions in the body. The bursa normally contains only a trace of fluid; when inflamed it can swell dramatically, forming a painless or painful fluctuant mass at the elbow tip. It is visible, easily palpable, and often cosmetically concerning to patients.
Types & Causes
|
Traumatic Bursitis |
A direct blow or repetitive pressure on the olecranon (student’s elbow, miner’s elbow) — fluid accumulates from bursal haemorrhage and mechanical irritation |
|
Inflammatory Bursitis |
Associated with rheumatoid arthritis, gout (tophi can deposit in the bursal wall — olecranon is the most common site for tophus formation), pseudogout |
|
Septic Bursitis |
Bacterial infection — most commonly Staphylococcus aureus via skin abrasion or puncture wound over the bursa. Presents with warmth, erythema, tenderness, and fever. Requires aspiration and antibiotics. Must be distinguished from inflammatory bursitis by aspiration and culture. |
|
Idiopathic Bursitis |
No identifiable cause in approximately 30% of cases |
Symptoms
- Visible swelling at the olecranon tip: May be painless (traumatic/inflammatory) or markedly tender (septic)
- Pain when leaning on the elbow or bending the elbow fully
- Warmth and erythema: Present in septic and acute inflammatory bursitis — requires aspiration to exclude infection
- Full range of elbow motion is typically preserved (unlike elbow joint pathology)
Diagnosis & Treatment
- Clinical diagnosis is usually straightforward. Aspiration: Essential when septic bursitis is suspected — fluid sent for cell count, culture, sensitivity, and crystal microscopy.
- Aspiration alone (non-septic): Successful in approximately 50% of non-septic cases. Often recurs without addressing the underlying cause.
- Corticosteroid injection (non-septic, inflammatory): Combined aspiration and steroid injection is effective for inflammatory and recurrent traumatic bursitis. Avoid in septic bursitis.
- Antibiotics (septic): Oral flucloxacillin for mild septic bursitis; IV antibiotics and surgical drainage for severe or non-responding infection.
- Surgical excision (bursectomy): For recurrent or chronic bursitis failing conservative measures, or chronic septic bursitis with scarred bursal walls. Small posterior incision; day-case procedure. Excellent results.
Patient FAQs –Olecranon Bursitis
My elbow has swelled but doesn't hurt much — should I be worried?
Painless swelling at the olecranon tip is very common and is usually traumatic or idiopathic bursitis. It can look alarming but is rarely serious. However, any swelling accompanied by warmth, redness, fever, or tenderness should be assessed promptly to exclude septic bursitis, which requires antibiotic treatment.
Will the swelling go away on its own?
Mild traumatic bursitis often resolves spontaneously over 4–8 weeks with elbow padding and avoidance of pressure. Larger bursal collections and inflammatory bursitis usually require aspiration and/or injection for resolution.
















