
Cubital Tunnel Syndrome (Ulnar Nerve Compression)
Overview & Anatomy
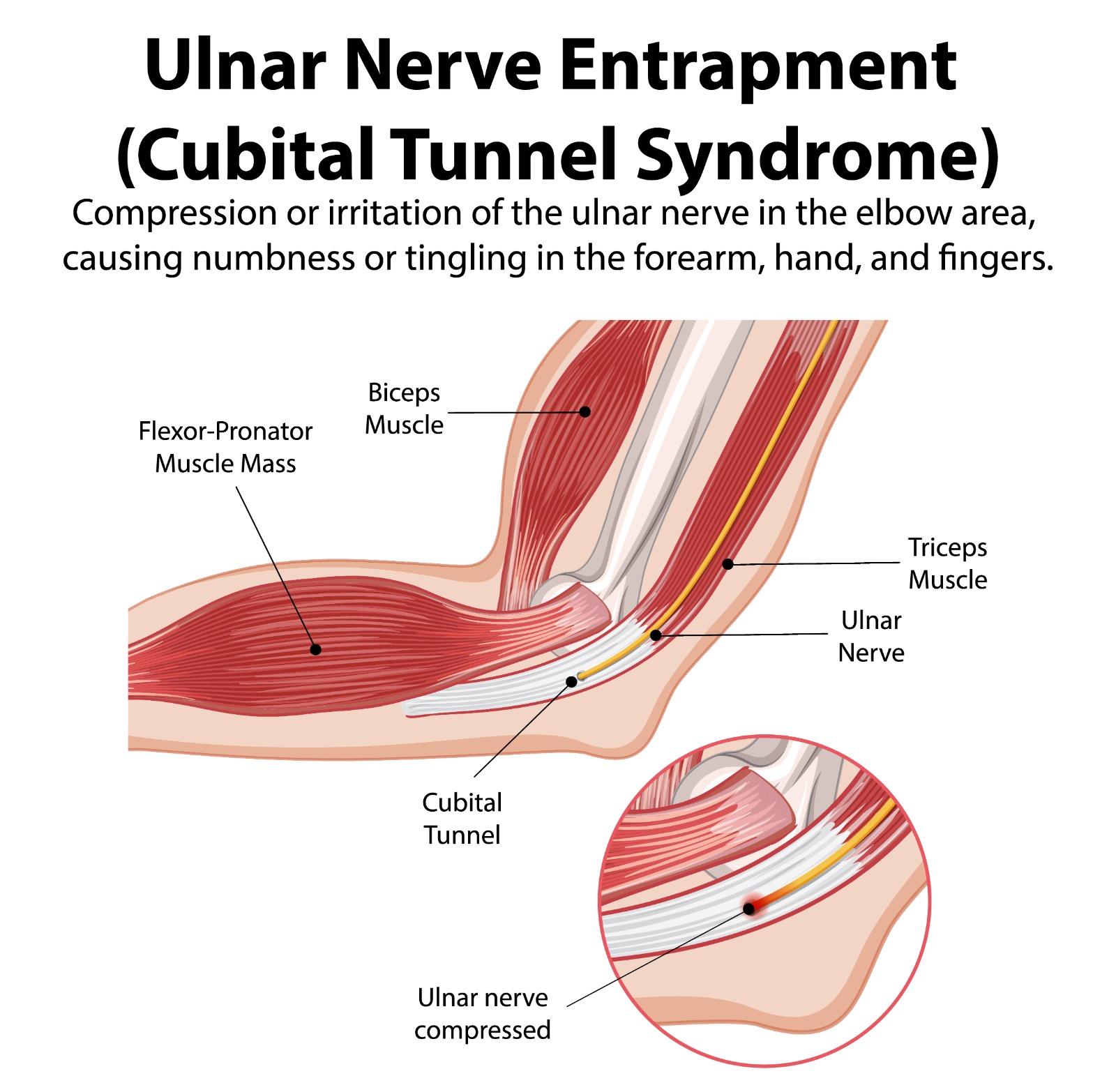
Cubital tunnel syndrome is the second most common peripheral nerve compression syndrome in the upper limb (after carpal tunnel syndrome), accounting for the vast majority of ulnar nerve compression presentations. The ulnar nerve passes through the cubital tunnel — a fibro-osseous channel on the posteromedial aspect of the elbow, bounded by the medial epicondyle anteriorly and the olecranon posteriorly, covered by the Osborne ligament (arcuate ligament of the cubital tunnel).
The nerve is vulnerable at this site because: (1) it takes the longest excursion of any peripheral nerve with elbow flexion and extension (up to 1.5 cm); (2) the cubital tunnel narrows by 55% during full elbow flexion, compressing the nerve; and (3) the nerve lies directly beneath the skin with minimal soft tissue protection, making it vulnerable to external pressure.
Causes & Risk Factors
- Prolonged or repetitive elbow flexion: Sleeping with the elbow fully bent, prolonged desk work with elbows flexed (particularly common with mobile phone use), and occupational elbow flexion
- Direct external compression: Leaning on the elbow on hard surfaces; prolonged operative positioning
- Elbow arthritis / osteophytes: Bony spurs within the cubital tunnel directly compress the nerve
- Cubitus valgus deformity: Increased carrying angle following childhood lateral condyle fractures — produces a slowly progressive ‘tardy’ ulnar nerve palsy decades after injury
- Medial epicondyle anomaly or snapping ulnar nerve: Subluxation of the nerve over the medial epicondyle during elbow flexion, causing repeated stretch injury
- Ganglia, lipomas, or tumours: Space-occupying lesions in the cubital tunnel
Symptoms
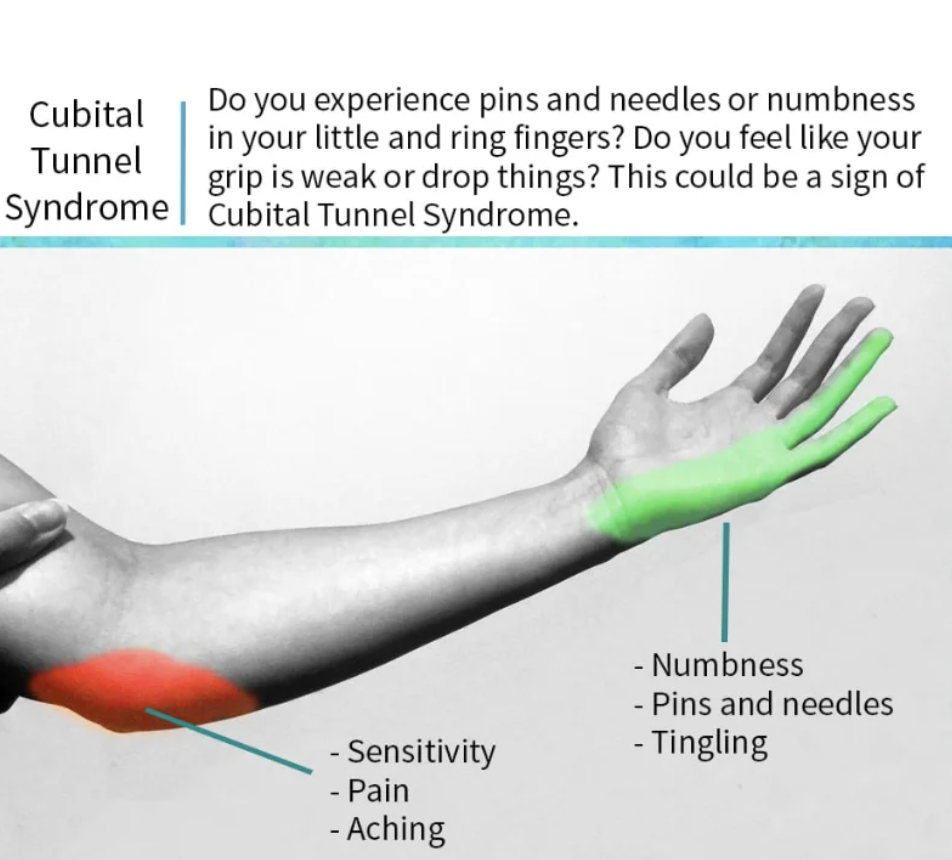
- Paraesthesia (tingling, numbness) in the ring and little fingers — the classic distribution of ulnar sensory supply to the hand
- Symptoms typically worse with elbow flexion (driving, phone use, sleeping) and improve with elbow extension
- Intrinsic muscle weakness: Weakness of the interossei (finger abduction/adduction), hypothenar muscles (little finger opposition and abduction), and adductor pollicis (thumb adduction)
- Clawing of the ring and little fingers: Intrinsic minus posture from loss of ulnar-innervated lumbrical and interosseous muscle function — a sign of advanced denervation
- Froment’s sign: Thumb IP flexion to compensate for weak adductor pollicis when pinching — pathognomonic of ulnar nerve weakness
- Wasting of the first dorsal interosseous (the web space between thumb and index finger) and hypothenar eminence — visible in established cases
Diagnosis
Tinel’s Sign | Percussion of the ulnar nerve at the medial epicondyle reproduces tingling in the ring and little fingers |
Elbow Flexion Test | Full elbow flexion with wrist extended for 60 seconds reproduces symptoms — sensitivity ~75% |
Scratch Collapse Test | Loss of external rotation resistance with simultaneous scratch over the nerve — indicates nerve sensitisation |
Grip & Pinch Strength | Dynamometry documents the degree of weakness for baseline and outcome measurement |
Investigations
- Nerve conduction studies (NCS) and electromyography (EMG): Gold standard investigation. Confirm the site of compression, quantify the degree of axonal loss, and identify concurrent proximal (thoracic outlet, cervical spine) or distal (Guyon’s canal) compression. Essential before surgical planning.
- X-ray elbow: Excludes bony pathology contributing to compression (osteophytes, heterotopic ossification, malunion)
- MRI or ultrasound: Identifies compressive lesions (ganglia, lipomata), assesses nerve calibre and signal change, and quantifies intrinsic muscle atrophy
Treatment
Non-Surgical (Mild–Moderate Cases)
- Elbow extension night splint: Prevents sustained elbow flexion during sleep — the single most effective conservative intervention. A 20–30° flexion night splint for 3–6 months provides relief in mild-to-moderate cases.
- Activity and posture modification: Avoiding prolonged elbow flexion, elbow padding, and adjusting workstation ergonomics
- Physiotherapy: Nerve gliding exercises and posture retraining
Key Point: Non-surgical treatment is appropriate for mild and moderate cubital tunnel syndrome (intermittent paraesthesia, no weakness, normal or mildly abnormal NCS). Established muscle weakness, marked sensory deficit, or severe NCS abnormality are indications for early surgical intervention — nerve recovery after long-standing denervation is incomplete.
Surgical Treatment
Surgery is highly effective for moderate-to-severe cubital tunnel syndrome. Dr. Senthilvelan’s approach:
- Simple decompression (neurolysis): The Osborne ligament and surrounding fascial bands are released, freeing the nerve without disturbing its bed. Best for compression without subluxation. Minimal recovery.
- Anterior transposition (subcutaneous, intramuscular, or submuscular): The ulnar nerve is rerouted to lie anterior to the medial epicondyle, eliminating the stretch mechanism and the compression. Preferred for recurrent cases, subluxing nerve, medial epicondyle anomaly, and cases with significant tension-related pathology. Submuscular transposition provides the most protected environment but requires longer recovery.
- Medial epicondylectomy: Partial removal of the medial epicondyle to decompress the nerve — less commonly performed; retained as an option for specific anatomical situations.
Patient FAQs –Cubital Tunnel Syndrome (Ulnar Nerve Compression)
Will my finger numbness go away after surgery?
Sensory recovery after cubital tunnel decompression is reliable in mild and moderate cases — most patients experience progressive resolution of tingling and numbness within 3–6 months. Muscle weakness recovery is slower (6–18 months) and depends on the duration of compression before surgery. Established muscle wasting may not fully recover. Early surgery gives the best functional outcome.
Is cubital tunnel surgery a major operation?
No — simple decompression is performed under local anaesthesia or light sedation as a day-case procedure. Anterior transposition requires a small incision and is usually day-case under regional block. Most patients return to light activities within 1–2 weeks and full activities within 4–6 weeks.
Can I prevent cubital tunnel syndrome from worsening?
Yes. Avoiding prolonged elbow flexion — particularly at night — using a night extension splint, adjusting your workspace to keep elbows in a neutral position, and avoiding leaning on the medial elbow are all effective in halting progression of mild-to-moderate disease. If weakness has developed, surgery is recommended promptly to protect remaining nerve function.
















