
Elbow Osteoarthritis
Overview & Anatomy
Elbow osteoarthritis is less common than hip, knee, or shoulder arthritis because the elbow carries predominantly compressive rather than shear loads during most daily activities. However, it causes significant disability when it does occur — particularly in heavy manual workers and throwing athletes who have subjected the joint to decades of high loading. Primary elbow OA most commonly affects dominant-arm manual workers (miners, blacksmiths, heavy machine operators) and is characterised by osteophyte formation at the olecranon tip and coronoid process, rather than the diffuse joint space narrowing seen in other joints.
Types of Elbow Arthritis
Primary Osteoarthritis | Degenerative cartilage loss — dominant arm heavy manual workers. Osteophytes at olecranon/coronoid tips cause terminal flexion and extension block. Joint space relatively preserved until late. |
Post-Traumatic Arthritis | Following intra-articular fractures, dislocations, or ligament injuries. Accelerated degeneration from malunion, chondral damage, and altered joint mechanics. Can affect any age group. |
Rheumatoid Arthritis | Bilateral, symmetrical synovitis with progressive joint destruction. Carries risk of spontaneous distal humerus fracture in longstanding cases due to severe bone erosion and osteopaenia. |
Crystal Arthropathy (Gout/Pseudogout) | Acute flares of severe elbow pain and swelling from urate or calcium pyrophosphate crystal deposition. Identified by aspiration and crystal microscopy. |
Symptoms
- Terminal range pain and stiffness: Pain and block at the limits of flexion and extension — the classic presentation of primary OA osteophytes impinging within the joint
- Loss of terminal extension: Inability to fully straighten the elbow is the earliest and most functionally limiting finding. Normal elbow extension = 0°; OA patients may lose 10–30°.
- Locking and catching: Loose bodies (osteophyte fragments) in the joint cause sudden locking with severe pain, requiring manipulation to unlock
- Crepitus: Audible or palpable grating during elbow movement
- Ulnar nerve symptoms: Osteophytes in the cubital tunnel can compress the ulnar nerve — presenting with ring and little finger numbness and tingling
Diagnosis
- Clinical examination: Specific assessment of flexion/extension arc, forearm rotation, crepitus, and ulnar nerve function
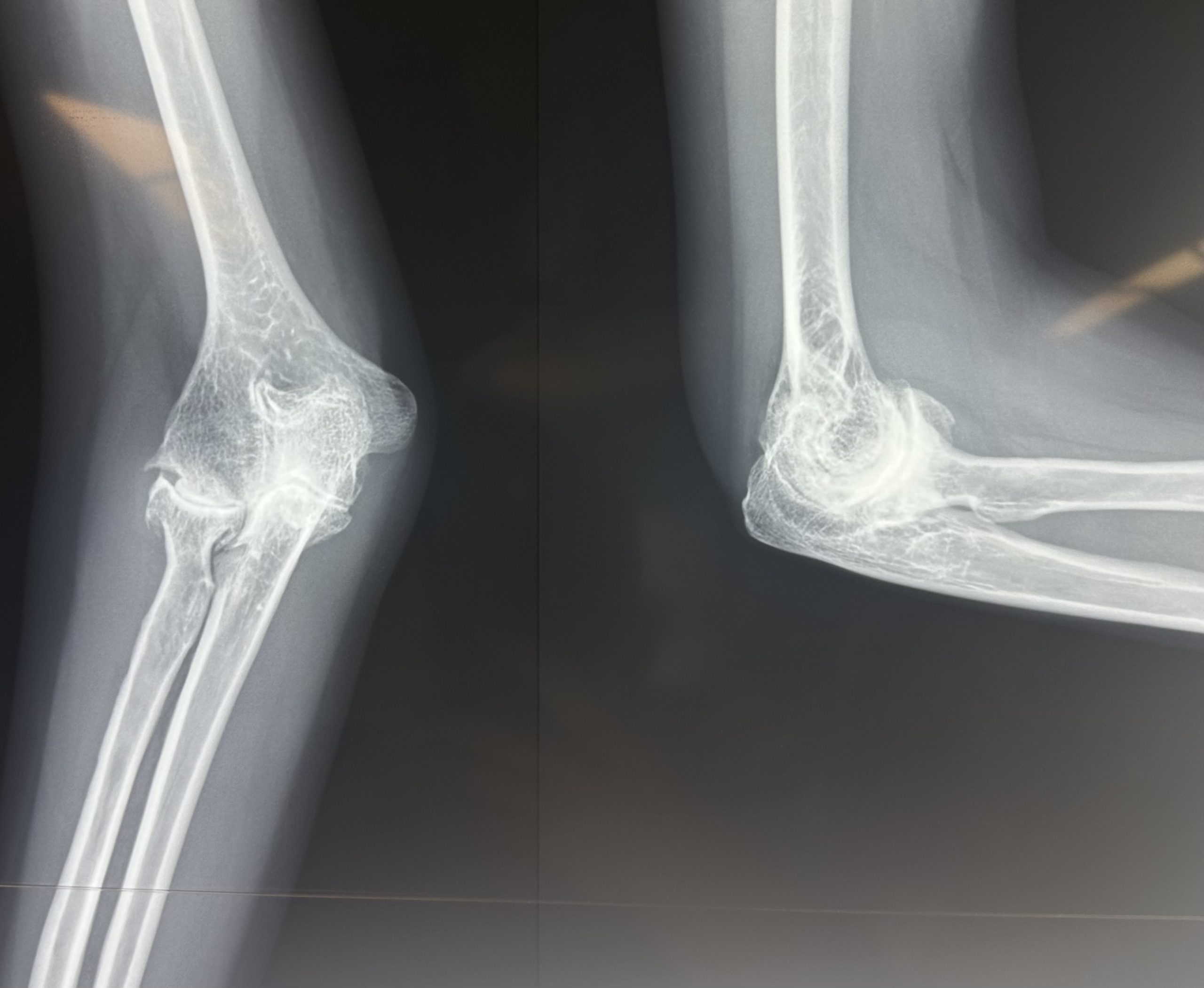
- Plain X-ray: AP and lateral views. Shows osteophytes at olecranon tip and coronoid process, loose bodies, joint space narrowing in advanced disease
- CT scan: Essential for surgical planning — precisely defines osteophyte size and location, loose body number and position, and the degree of joint space narrowing
- MRI: Used when cartilage assessment, ulnar nerve evaluation, or osteochondral defect characterisation is required
Treatment
Non-Surgical
- Activity modification: Avoiding extreme ranges of motion and heavy loading during symptomatic flares
- Physiotherapy: Maintaining range of motion; eccentric strengthening to offload the joint
- NSAIDs and analgesics: For pain management
- Intra-articular corticosteroid injection: Useful for inflammatory flares — particularly in rheumatoid and crystal arthritis. Guided by ultrasound or fluoroscopy.
- Disease-modifying therapy (RA): Rheumatological co-management with DMARDs and biologics is the cornerstone of rheumatoid elbow management
Surgical Treatment
- Arthroscopic elbow debridement and osteophyte resection (Outerbridge-Kashiwagi procedure): The keyhole operation of choice for primary OA. Osteophytes are removed from the olecranon tip (through the posterior compartment) and coronoid tip (through the anterior compartment), loose bodies are retrieved, and the joint is lavaged. Restores terminal range of motion with high patient satisfaction. Most patients gain 15–25° of additional arc. Day-case or overnight procedure.
- Open debridement: For extensive osteophytes or cases requiring simultaneous ulnar nerve decompression
- Total elbow replacement (arthroplasty): For end-stage arthritis with severe pain and bone destruction.
Post OP Elbow Replacement
Patient FAQs –Elbow Osteoarthritis
My elbow suddenly locks and I cannot straighten it — what should I do?
Sudden locking is caused by a loose body (fragment of bone or cartilage) wedging itself within the joint. It usually resolves with gentle manipulation — avoid forcing the movement. This symptom is a strong indication for arthroscopic loose body removal. Please contact Dr. Senthilvelan’s clinic for an early assessment.
Can elbow arthritis affect my ability to work?
Yes — loss of terminal extension significantly impairs load-bearing, overhead work, and fine motor precision tasks. Following arthroscopic debridement, most patients regain a functional arc (30–130°) sufficient for the majority of occupational and daily activities. Dr. Senthilvelan can provide a workplace modification letter during the recovery phase.
















