")
Lateral Epicondylitis (Tennis Elbow)
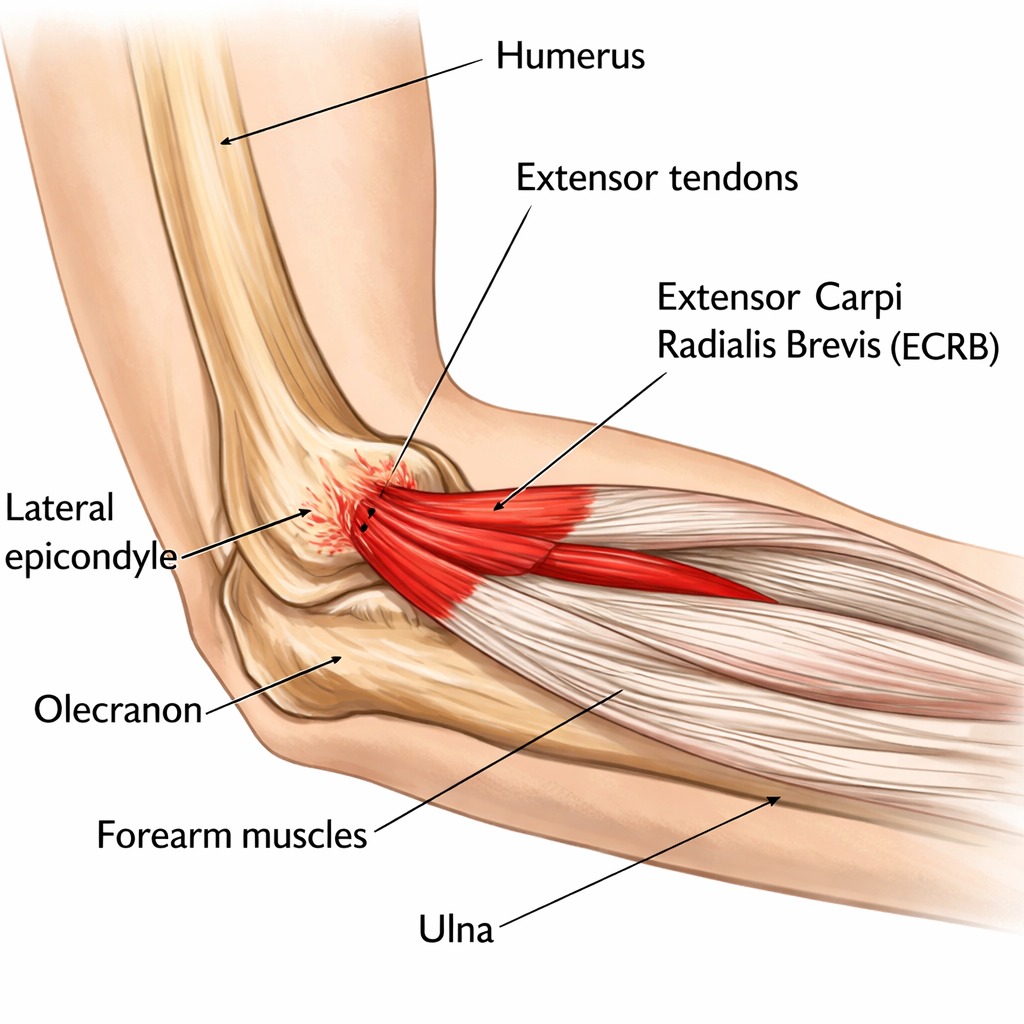
Overview & Anatomy
Lateral epicondylitis — commonly known as tennis elbow — is the most frequently encountered elbow condition in orthopaedic and sports medicine practice, affecting approximately 1–3% of the general population. Despite the name, only 5–10% of sufferers are tennis players. It is a condition of the common extensor origin at the lateral epicondyle of the humerus, where the wrist and finger extensor muscles (most critically the extensor carpi radialis brevis, or ECRB) attach.
Histological studies consistently demonstrate that the pathology is not primarily inflammatory but rather angiofibroblastic tendinosis — a degenerative process characterised by disorganised collagen, immature fibroblast infiltration, and absence of inflammatory cells. This understanding has shifted treatment philosophy away from anti-inflammatory strategies toward tendon regeneration and load management.
Causes & Risk Factors
- Repetitive wrist extension and gripping activities — particularly those combining forearm rotation with wrist extension
- Occupational exposure: Plumbers, painters, carpenters, computer users, chefs, and manual workers
- Sporting activities: Racket sports (improper backhand technique), golf (impact phase), fishing, and rowing
- Age: Peak incidence 40–50 years, coinciding with the period of peak degenerative tendon change
- Dominant arm: 75% of cases affect the dominant limb
- Prior corticosteroid injection: Paradoxically, repeated injections may promote further tendon degeneration
Symptoms & Clinical Presentation
- Lateral elbow pain: Localised to the lateral epicondyle, often radiating down the forearm extensor compartment toward the wrist
- Aggravating activities: Gripping, lifting, carrying, using tools, opening jars, shaking hands, and typing
- Point tenderness: Precisely located 1–2 cm distal to the lateral epicondyle over the ECRB origin — the most reliable clinical sign
- Pain with resisted wrist extension: The hallmark test — pain reproduced by resisting dorsiflexion of the wrist with the elbow fully extended (Cozen’s test / Mills’ test)
- Grip strength reduction: Dynamometry typically shows 20–30% reduction compared to the contralateral side
- Night pain and rest pain in severe cases
Diagnosis
Clinical Tests
Cozen’s Test | Elbow extended, forearm pronated, wrist in neutral — patient resists active wrist extension. Positive if reproduces lateral epicondyle pain. |
Mill’s Test | Elbow extended, forearm pronated, wrist passively flexed. Pain at lateral epicondyle = positive. |
Chair Test | Patient attempts to lift a chair with the elbow extended and forearm pronated. Reproduces pain. |
Maudsley’s Test | Resisted middle finger extension with elbow extended — stresses ECRB specifically. |
Imaging
- X-ray: Usually normal. May show calcification at the lateral epicondyle in chronic cases. Useful to exclude elbow arthritis or loose bodies.
- Ultrasound: First-line imaging. Shows tendon thickening, hypoechoic change, intratendinous tears, and neovascularity (Doppler). Guides therapeutic injections.
- MRI: Used for surgical planning or diagnostic uncertainty. T1 and T2 changes in the ECRB at its epicondylar origin; may show partial or complete tendon tears.
Treatment
Conservative Management (First-Line — 80–90% of patients respond)
- Activity modification: Identify and reduce provocative loading. Temporary avoidance of gripping-intensive tasks.
- Counterforce (epicondyle) brace: A strap worn 2–3 cm below the lateral epicondyle reduces tensile load on the ECRB origin. Provides symptomatic relief for many patients during activity.
- Physiotherapy: The cornerstone of treatment. Eccentric and isometric wrist extensor strengthening exercises (particularly Tyler Twist and Theraband FlexBar programme) have strong evidence for reducing pain and improving strength. Progressive tendon loading is the most effective strategy.
- NSAIDs / topical diclofenac: Short-term pain relief. Topical application directly over the epicondyle is well-tolerated and avoids systemic side effects.
- Corticosteroid injection: Provides rapid short-term (4–8 week) pain relief but does not improve outcomes at 6–12 months compared to physiotherapy alone. Repeated injections are associated with higher long-term recurrence rates — limited to 1–2 injections maximum.
- Platelet-Rich Plasma (PRP) injection: Growing evidence supports PRP for chronic tennis elbow refractory to other measures. Single injection with structured rehabilitation. Better medium-term outcomes than corticosteroid in randomised trials.
- Extracorporeal Shock Wave Therapy (ESWT): Non-invasive ultrasound-based energy delivery to stimulate tendon healing. Recommended for chronic cases (>3 months) failing other non-surgical treatment. 3–6 sessions.
Surgical Treatment

Surgery is considered in fewer than 10% of cases, after a minimum 6–12 months of comprehensive non-surgical management:
- Arthroscopic debridement and ECRB release: Dr. Senthilvelan’s preferred technique. Arthroscopic resection of the degenerative ECRB tissue and release of its origin under direct visualisation. Allows simultaneous assessment and treatment of intra-articular pathology (cartilage, loose bodies, plica). Day-case procedure with sling for 1–2 weeks.
- Open ECRB release and debridement: Alternative for cases not amenable to arthroscopic technique. Small 3–4 cm lateral incision; equivalent outcomes to arthroscopic approach.
- Recovery after surgery: Return to light activities at 2–4 weeks; strengthening physiotherapy from 4 weeks; return to manual work and sport at 3–6 months.
Patient FAQs – Lateral Epicondylitis (Tennis Elbow)
How long does tennis elbow take to get better?
With consistent physiotherapy and activity modification, 80–90% of patients recover within 12 months. Early cases with prompt treatment may resolve in 3–6 months. Chronic cases — particularly those who have received multiple steroid injections — may take 12–24 months. Patience and adherence to the loading programme are the most important prognostic factors.
Is a steroid injection the best treatment?
Corticosteroid injection provides excellent short-term pain relief but multiple randomised controlled trials — including the landmark PETRA and NICE trials — have demonstrated that steroid injection produces worse outcomes at 6–12 months compared to physiotherapy alone and watchful waiting. Dr. Senthilvelan limits its use to acute flares that are preventing engagement with rehabilitation.
Will tennis elbow keep coming back?
Recurrence is common if the underlying biomechanical cause — typically a combination of overload, poor technique, and weak muscles — is not addressed. Completing the full physiotherapy programme, correcting technique in sport, and modifying occupational loading significantly reduces recurrence risk.
Do I need an MRI for tennis elbow?
MRI is not routinely required for diagnosis. A careful clinical examination with the tests described above is sufficient in most cases. MRI is reserved for cases where diagnosis is uncertain, symptoms are atypical, surgery is being planned, or where intra-articular pathology needs exclusion.
















