")
Thumb Basal Joint Arthritis (CMC Arthritis)
Overview
Arthritis of the carpometacarpal (CMC) joint of the thumb — the basal joint — is the most common site of hand arthritis, affecting up to 15% of post-menopausal women. The CMC joint is a saddle-shaped joint at the base of the thumb that allows the wide range of thumb motion essential for pinch and opposition. It bears extraordinary forces during pinching — up to 13 times the applied pinch force is transmitted across the CMC joint. This high mechanical loading, combined with the laxity-prone beak ligament, drives early degenerative change.


Symptoms & Eaton Staging
CMC arthritis presents along a spectrum from ligamentous laxity in young patients to end-stage bone-on-bone arthritis in older patients. The Eaton-Littler radiographic staging system guides treatment:
Stage I | Normal joint space. Synovitis and ligamentous laxity only. Treated conservatively. |
Stage II | Joint space narrowing <1/3. Small osteophytes. Subchondral sclerosis. Conservative treatment; injection highly effective. |
Stage III | Joint space narrowing >1/3. Large osteophytes. Adduction of the first metacarpal. Conservative treatment failing; surgical intervention likely. |
Stage IV | Complete joint destruction, involving STT joint. Surgical treatment required. |
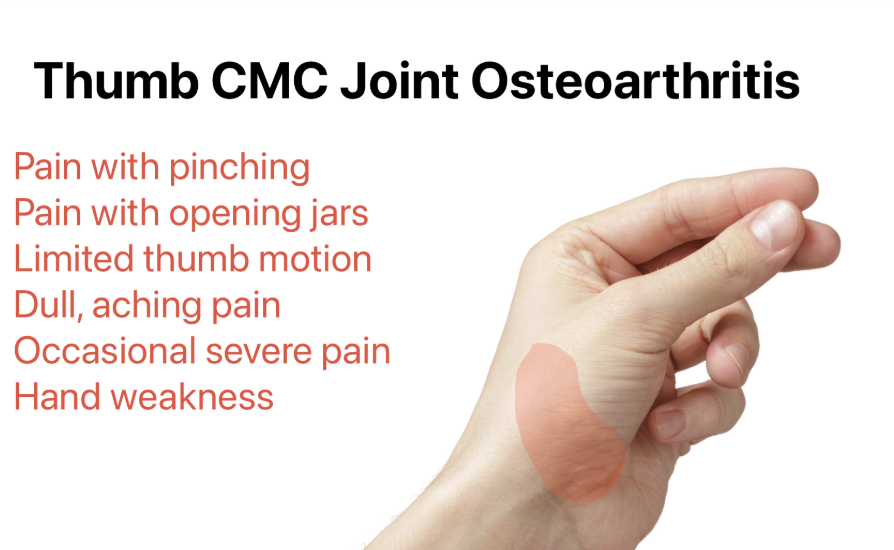
- Pain at the base of the thumb, aggravated by pinching, gripping, opening jars, turning keys, and using scissors
- Tenderness directly over the CMC joint — the ‘grind test’ (axial compression with rotation of the first metacarpal) reproduces pain and is pathognomonic
- Characteristic ‘Z-deformity’ of the thumb in advanced cases: CMC subluxation + compensatory hyperextension of the MCP joint
- Weakness of pinch — ‘dropping things’ and inability to open packaging
Treatment
Non-Surgical
- Thumb spica splint: A hand-based splint immobilising the CMC joint while leaving the IP joint free. Reduces pain during activities significantly. Long-term splint use during provocative tasks.
- Corticosteroid injection: Highly effective in Stages I–III. Ultrasound-guided injection into the CMC joint. Provides reliable relief for 2–6 months. Can be repeated. Hyaluronic acid viscosupplementation is an alternative for patients preferring to minimise steroid use.
- Physiotherapy: Joint protection strategies, strengthening of the thenar and intrinsic muscles, activity modification
Surgical Treatment
Surgery is recommended when non-surgical measures provide insufficient relief, typically for Stage III–IV disease:
- Trapeziectomy with ligament reconstruction and tendon interposition (LRTI): The traditional gold standard. The trapezium bone (which forms the socket of the CMC joint) is excised, eliminating the arthritic joint. A portion of the flexor carpi radialis or abductor pollicis longus tendon is used to fill the space and reconstruct the ligament. Excellent long-term pain relief and thumb function.
- Trapeziectomy alone: Simpler procedure with equivalent long-term outcomes to LRTI in randomised trials — current evidence does not support the routine addition of tendon reconstruction. Increasing preference for simple trapeziectomy in contemporary practice.
- CMC joint replacement (arthroplasty): Total joint replacement preserving motion and thumb length. Promising intermediate results but longer-term implant survival data awaited.
- Recovery: Thumb spica cast for 4–6 weeks; physiotherapy for 3–6 months; full recovery at 6–12 months. Outcomes: >90% of patients report significant pain relief and functional improvement.
Patient FAQs – Thumb Basal Joint Arthritis (CMC Arthritis)
Is thumb arthritis surgery worth it?
Yes — for patients with moderate-to-severe CMC arthritis that has failed conservative treatment, trapeziectomy has excellent outcomes. Over 90% of patients are satisfied with their results at 5 and 10 year follow-up. Pain relief is reliable; strength recovery takes 6–12 months but most patients return to all activities including sport and manual work.
How long does the recovery take after trapeziectomy?
You will be in a thumb spica cast for 4–6 weeks, followed by 3–6 months of physiotherapy. Most patients return to light daily activities at 6–8 weeks, driving at 8–10 weeks, and full manual work and sport at 6–12 months. The thumb will feel different for up to 2 years as the body adapts to the absence of the trapezium.