Scaphoid Fracture
Overview & Importance
The scaphoid is the most commonly fractured carpal bone, accounting for approximately 60–70% of all carpal fractures. It occupies a pivotal position spanning both carpal rows and is the primary load-bearing bone of the wrist. Despite being a small bone, scaphoid fractures carry an outsized clinical significance because of the scaphoid’s unique and precarious blood supply — the entire proximal pole (up to 70–80% of the bone) is supplied by a single retrograde vessel entering distally, making proximal pole fractures highly susceptible to avascular necrosis (bone death) and non-union.
Critical Warning: A scaphoid fracture that is not treated promptly and correctly has a high risk of progressing to non-union and avascular necrosis — ultimately causing the SNAC wrist collapse pattern described in Chapter 4, producing severe, disabling arthritis within 10–20 years. Early diagnosis and appropriate treatment are essential.
Mechanism & Presentation
- Mechanism: Fall onto an outstretched hand (FOOSH) with the wrist in extension and radial deviation — the classic mechanism transmitting force across the scaphoid waist
- Most common in young active males aged 15–35
- Clinical presentation: ‘Anatomical snuffbox’ tenderness (the dorsoradial triangular depression between EPL and EPB/APL) is the most sensitive sign — if present, treat as scaphoid fracture until proven otherwise
- Pain with axial compression along the thumb ray (scaphoid compression test)
- The diagnosis is frequently missed on initial X-ray: plain films miss approximately 20% of acute scaphoid fractures — do not rely on a negative X-ray to exclude the diagnosis in a patient with snuffbox tenderness
Fracture Classification
Distal Pole | 20% of fractures. Excellent blood supply. Heals reliably with cast immobilisation. |
Waist (Middle Third) | 70% of fractures. Intermediate vascularity. Undisplaced fractures can be managed non-surgically but surgical fixation allows faster return to activity. |
Proximal Pole | 10% of fractures. Most precarious blood supply. High risk of AVN. Surgical fixation strongly recommended. |
Diagnosis
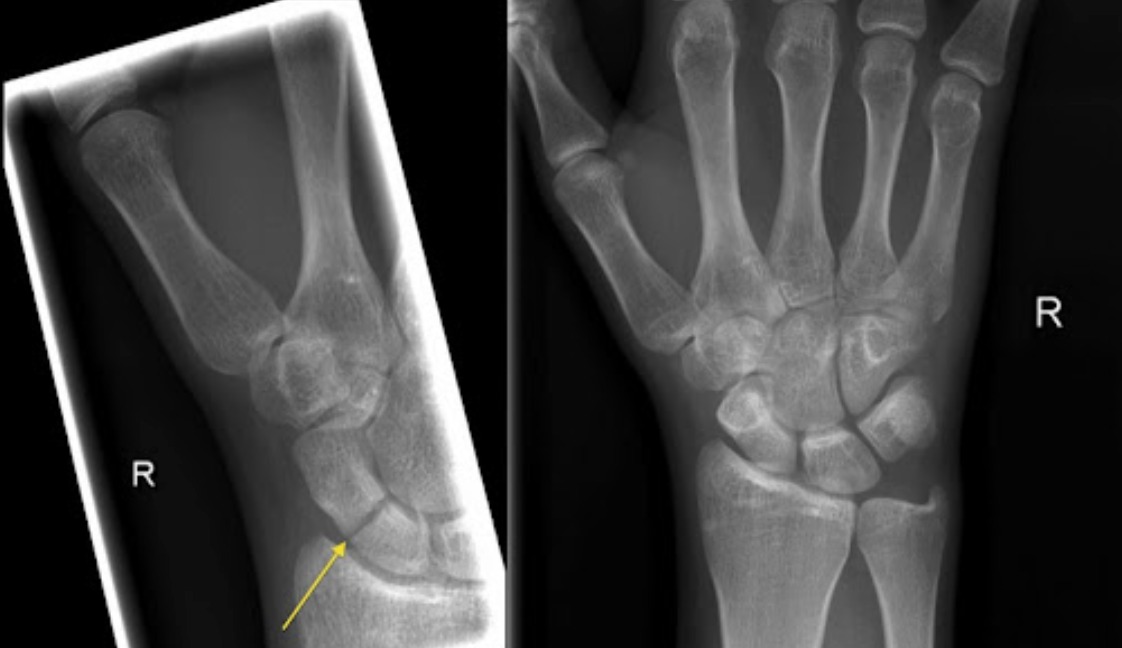
- Initial X-ray: AP, lateral, and scaphoid views (scaphoid oblique). Sensitivity only ~70% acutely — a negative X-ray does not exclude fracture.
- MRI: The gold standard for diagnosing occult (X-ray negative) scaphoid fractures and for assessing vascularity (avascular necrosis). Performed within 1–2 weeks of injury for diagnostic certainty.
- CT scan: Superior for fracture classification, displacement measurement, and assessing union in known fractures. Essential for surgical planning.
Treatment
Undisplaced Fractures
- Non-surgical (cast immobilisation): A below-elbow scaphoid cast or thumb spica cast worn for 8–12 weeks. Effective for undisplaced distal pole and waist fractures. Delayed union risk increases the longer the time from injury to treatment.
- Percutaneous screw fixation: Increasingly preferred even for undisplaced waist fractures in active patients and manual workers — allows earlier return to work and sport (6–8 weeks vs 10–12 weeks), higher union rate, and avoids the inconvenience and muscle wasting of prolonged casting.
Displaced Fractures (>1mm displacement, angulation, or instability)
- Surgical fixation is mandatory — displaced fractures have a >50% non-union rate with cast alone
- Open reduction and internal fixation (ORIF): Through a volar or dorsal approach depending on fracture pattern; a headless compression screw (Herbert, Acutrak, or similar) is inserted along the central axis of the scaphoid. Bone graft may be required for fractures with a humpback deformity.
Scaphoid Non-union
Untreated or failed fractures that fail to unite require reconstruction. The Matti-Russe procedure (inlay cancellous bone grafting) or the Zaidemberg vascularised bone graft (from the distal radius) is used for non-union without established AVN. For non-union with established AVN of the proximal pole, a vascularised graft from the medial femoral condyle is increasingly used.

Patient FAQs –Scaphoid Fracture
I fell on my wrist 2 weeks ago — it still hurts but X-rays were normal. Could it be a scaphoid fracture?
Yes, absolutely. Up to 20% of acute scaphoid fractures are not visible on initial X-ray. If you have anatomical snuffbox tenderness or pain with thumb axial loading, Dr. Senthilvelan will arrange an urgent MRI to confirm or exclude the diagnosis. Do not ignore persistent wrist pain after a fall.
How long does a scaphoid fracture take to heal?
Distal pole fractures typically heal in 6–8 weeks. Undisplaced waist fractures require 10–12 weeks in cast, or 6–8 weeks after surgical fixation. Proximal pole fractures may take 3–6 months even with surgery. Compliance with immobilisation or post-operative rehabilitation is crucial.
What happens if my scaphoid fracture doesn't heal?
Scaphoid non-union (failure to heal) leads to progressive wrist collapse and arthritis over years. Surgical intervention — bone grafting and screw fixation — is required. The earlier non-union is identified and treated, the better the outcome. This is why follow-up imaging is essential after any scaphoid fracture.