Ganglion Cysts
Overview
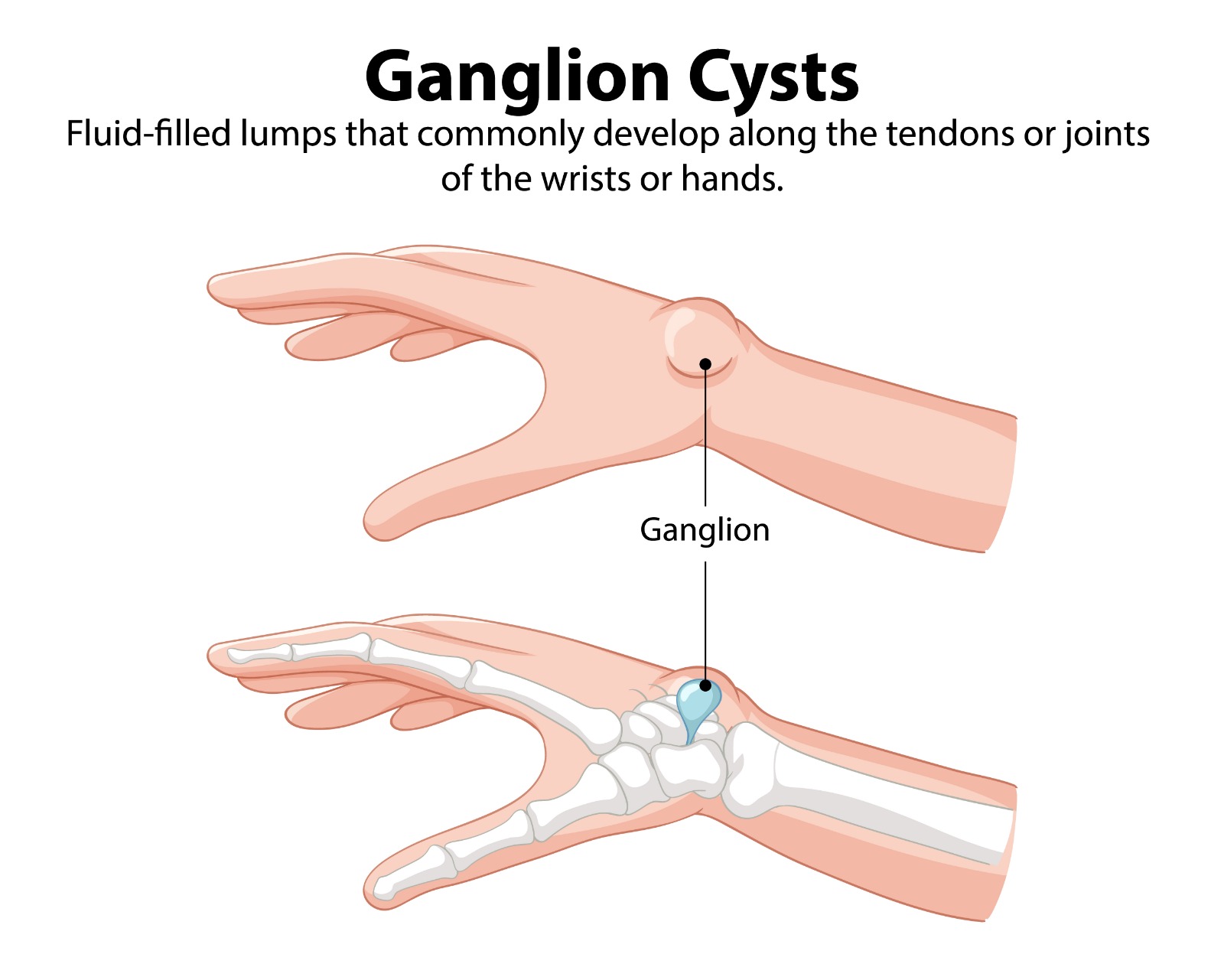
A ganglion cyst is the most common soft tissue mass of the hand and wrist, accounting for approximately 60–70% of all hand and wrist swellings. It is a benign, mucinous, fluid-filled cyst arising from the synovium of a joint or tendon sheath. The cyst communicates with the parent joint or sheath through a one-way valve-like pedicle, explaining why the cyst size fluctuates with activity and why aspiration alone has a high recurrence rate.
Common Locations
Dorsal Wrist (60–70%) | Arises from the scapholunate ligament. Visible and palpable on the dorsum of the wrist. May be firm and tense or soft and compressible. May transiently enlarge with wrist flexion. |
Volar Wrist (18–20%) | Arises from the radiocarpal joint or STT joint. Lies adjacent to the radial artery — must be assessed before aspiration or surgery. Firm, non-compressible. |
Flexor Tendon Sheath (10%) | A2 pulley level at the base of the finger — feels like a small hard pea. Tender on direct pressure. May cause triggering. |
Dorsal DIP Joint (Mucous Cyst) | Arises from the DIP joint — associated with underlying OA. Often produces a longitudinal nail groove. May discharge. |
Carpal Boss | Firm bony prominence at the base of the index or middle metacarpal — a CMC joint osteophyte, not a true ganglion. |
Symptoms
- Visible or palpable lump — may fluctuate in size from day to day or week to week
- May be completely asymptomatic (many are discovered incidentally)
- Aching or discomfort with wrist loading or extremes of motion
- Nerve compression: Volar wrist ganglia can compress the median or ulnar nerve; dorsal ganglia rarely cause nerve symptoms
- Large dorsal ganglia may cause wrist extension limitation
Diagnosis
Clinical diagnosis is usually straightforward. A round, smooth, transilluminable (light passes through) cyst is characteristic. Ultrasound confirms the cystic nature, identifies the pedicle, and assesses proximity to neurovascular structures. MRI is reserved for occult ganglia (clinically undetected, pain only) — the occult dorsal wrist ganglion is an important cause of unexplained dorsal wrist pain
Treatment
Observation
Approximately 50% of ganglia spontaneously regress without treatment. Observation is appropriate for asymptomatic ganglia or those causing only mild, tolerable symptoms. The traditional ‘Bible method’ (striking with a heavy book) is not recommended — it risks joint and soft tissue injury.
Aspiration
Needle aspiration of the ganglion contents (thick, gelatinous mucin) under local anaesthesia or ultrasound guidance. Technically simple and low-risk. Recurrence rate: 50–80% at 2 years — the pedicle is not addressed by aspiration. Appropriate as a first-line treatment for symptomatic ganglia, particularly while awaiting surgery.
Surgical Excision
- Excision of the ganglion with its pedicle and a cuff of the parent joint capsule or tendon sheath is the definitive treatment
- Recurrence rate after surgery: 5–15% (dorsal wrist) — significantly lower than aspiration
- Performed under local anaesthesia or regional block as a day-case procedure
- Dorsal wrist ganglion excision is increasingly performed arthroscopically — identifying and addressing the scapholunate origin directly, with smaller scars and equivalent recurrence rates
- Mucous cysts: Excision with debridement of the underlying DIP joint osteophyte. Often accompanied by skin grafting if the overlying skin is thin or eroded.

Patient FAQs – Ganglion Cysts
Is a ganglion cyst dangerous?
No — ganglion cysts are completely benign and do not become malignant. The primary indications for treatment are pain, cosmetic concern, nerve compression symptoms, or the patient’s own preference. If your lump has rapidly increased in size, is very hard, or is attached to bone, Dr. Senthilvelan will assess whether further investigation is needed to confirm the diagnosis.
Can a ganglion recur after being surgically removed?
Yes — recurrence after surgical excision occurs in 5–15% of dorsal wrist ganglia and up to 20% of flexor sheath ganglia. Complete excision of the pedicle and a cuff of the parent capsule minimises recurrence risk. Recurrent ganglia can be re-excised.