")
Distal Radius Fracture (Colles' & Barton's)
Overview
Distal radius fractures are among the most common fractures seen in both emergency and orthopaedic practice, accounting for approximately 17% of all fractures presenting to emergency departments. They occur predominantly in two distinct populations: young adults following high-energy trauma (falls from height, road traffic accidents, and sports) and elderly women with osteoporosis following low-energy falls onto an outstretched hand.

Classification & Fracture Types
Colles’ Fracture | The classic distal radius fracture — dorsal displacement and angulation with radial shortening. The wrist has a characteristic ‘dinner fork’ deformity. Most common fracture pattern in adults. |
Smith’s Fracture (Reverse Colles’) | Volar displacement of the distal fragment — the wrist appears ‘spade-shaped’. Caused by a fall onto the back of the hand. |
Barton’s Fracture | Intra-articular shear fracture of the dorsal (dorsal Barton’s) or volar (volar Barton’s) rim. The radiocarpal joint subluxes with the fragment — inherently unstable and almost always requires surgical fixation. |
Die-Punch Fracture | Depression of the lunate fossa of the radius — articular impaction. Requires anatomical reduction. |
Chauffeur’s Fracture | Radial styloid avulsion — historically associated with hand-crank injuries; now seen in falls and direct blows. |
Assessment
- Neurovascular examination: Acute carpal tunnel syndrome from haematoma and oedema compressing the median nerve occurs in 1–9% — presenting with acute hand numbness. Requires urgent reduction and monitoring.
- Radiographic assessment: AP and lateral wrist X-rays. Parameters critical for surgical decision-making: radial inclination (normal 22°), volar tilt (normal 11°), radial height (normal 11mm), and ulnar variance.
- CT scan: Mandatory for complex intra-articular fractures to characterise fragment displacement, step-off, and surgical planning.
Treatment
Acceptable Alignment — Non-Surgical
Many minimally displaced and well-reduced fractures in elderly lower-demand patients can be managed with cast immobilisation after closed reduction under haematoma block. Acceptable parameters: <5mm radial shortening, <5° dorsal angulation, <2mm articular step-off or gap.
Surgical Fixation
Surgery is recommended for fractures that are inherently unstable, that re-displace after closed reduction, or that involve complex intra-articular displacement:
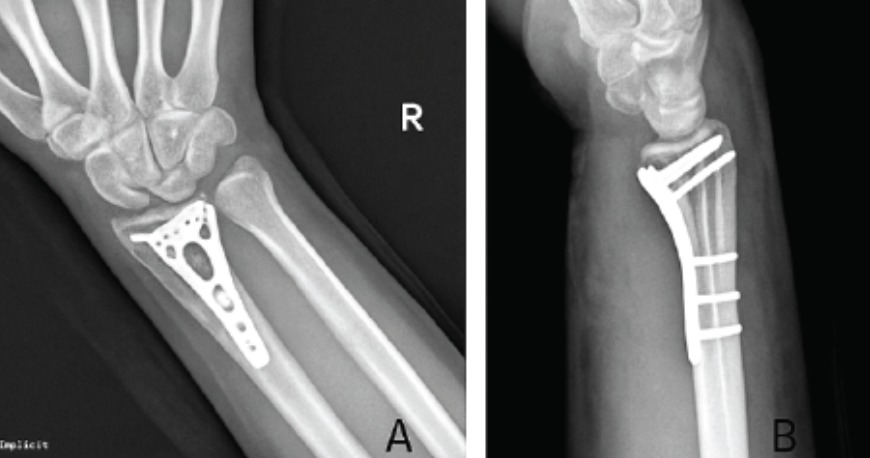
- Volar locking plate fixation (ORIF): The gold standard for surgical treatment of distal radius fractures. A pre-contoured plate is applied to the volar surface of the radius through a small anterior approach, capturing the distal fragments with locking screws that hold even in osteoporotic bone. Allows early mobilisation. Day case or overnight admission.
- Percutaneous K-wire fixation: Simpler technique for selected fracture patterns — adequate for some extra-articular fractures. Requires supplementary cast; wires removed at 4–6 weeks.
- External fixation: Used for highly comminuted fractures with significant soft tissue injury, or as a temporary measure before definitive plate fixation.
Recovery
0–2 weeks | Wound healing, elevation. Finger and shoulder exercises. |
2–6 weeks | Cast or splint removed (non-surgical or post-K-wire). Active wrist, forearm rotation exercises begin. |
6–12 weeks | Progressive strengthening. Return to light activities. |
3–6 months | Full wrist motion and grip strength recovery. Return to manual work and sport. |
Osteoporosis: A fragility fracture of the distal radius in a patient over 50 is a sentinel event indicating high fracture risk. Dr. Senthilvelan will refer patients for DEXA bone density scanning and osteoporosis treatment — preventing the next fracture is as important as treating the current one.
Patient FAQs –Distal Radius Fracture (Colles' & Barton's)
My wrist was put in a cast in A&E — do I need to see a specialist?
Yes. All displaced distal radius fractures should be reviewed by a hand or wrist surgeon within 1 week of injury to ensure the reduction has been maintained and that the fracture pattern is appropriate for non-surgical management. Re-displacement within the cast is common, and early identification allows conversion to surgical fixation before the fracture begins to consolidate in a poor position.
Will my wrist ever be fully normal?
Most patients with distal radius fractures recover excellent function. Complete recovery of wrist motion and grip strength typically takes 6–12 months. Articular fractures that were not perfectly reduced carry a small risk of developing post-traumatic arthritis long term. Anatomical reduction — whether by closed means or surgery — gives the best long-term outcome.