
Chronic Shoulder Instability
Treatment by Dr. Senthilvelan – Shoulder, Elbow & Wrist Specialist
Overview
The shoulder joint has the greatest range of motion of any joint in the body. It allows the arm to move overhead, behind the back, and in multiple directions. While this mobility is essential for daily activities and sports, it also makes the shoulder more vulnerable to instability.
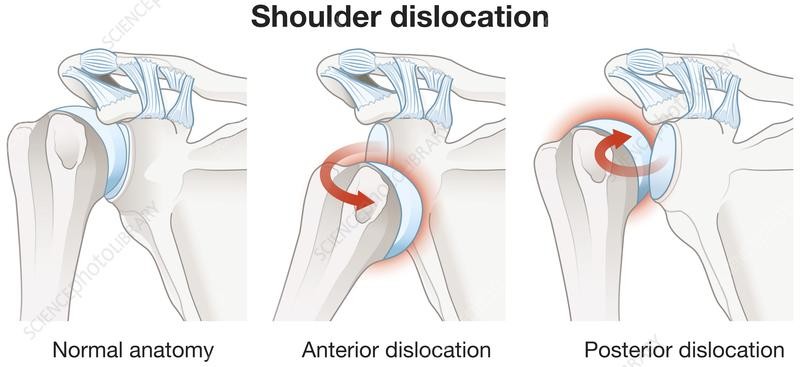
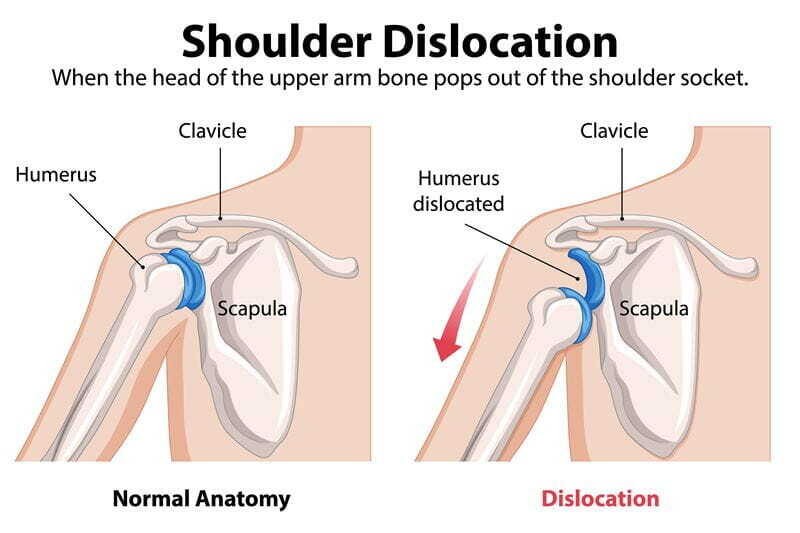
Shoulder instability occurs when the head of the humerus (upper arm bone) slips out of the glenoid (shoulder socket). This usually happens after a traumatic injury, such as a fall or accident.
Once a shoulder has dislocated, it becomes more prone to repeated dislocations. When the shoulder repeatedly slips out of place or feels loose, it is called chronic shoulder instability.
Dr. Senthilvelan specializes in treating shoulder instability using both advanced physiotherapy protocols and minimally invasive arthroscopic stabilization procedures.
Shoulder Anatomy
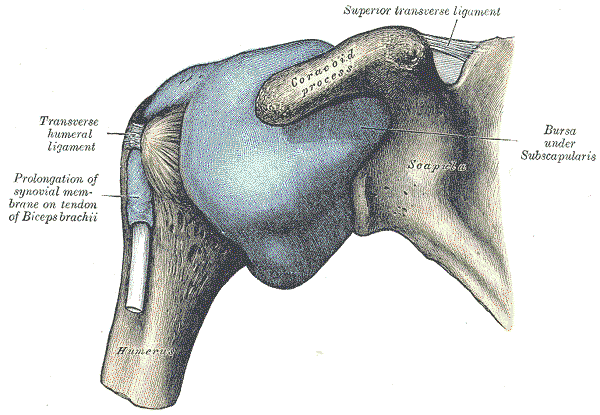
The shoulder is made up of three bones:
- Humerus (upper arm bone)
- Scapula (shoulder blade)
- Clavicle (collarbone)
The ball of the humerus fits into the shallow socket of the scapula, called the glenoid.
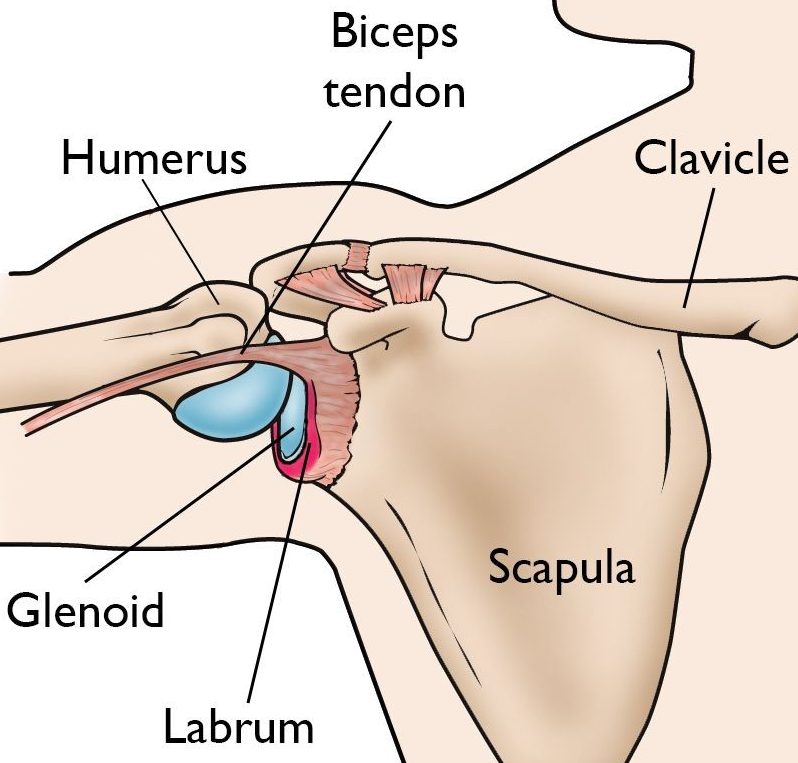
Stabilizing Structures
Shoulder stability depends on:
- Shoulder capsule: ligament system that surrounds the joint
- Labrum: cartilage rim that deepens the socket
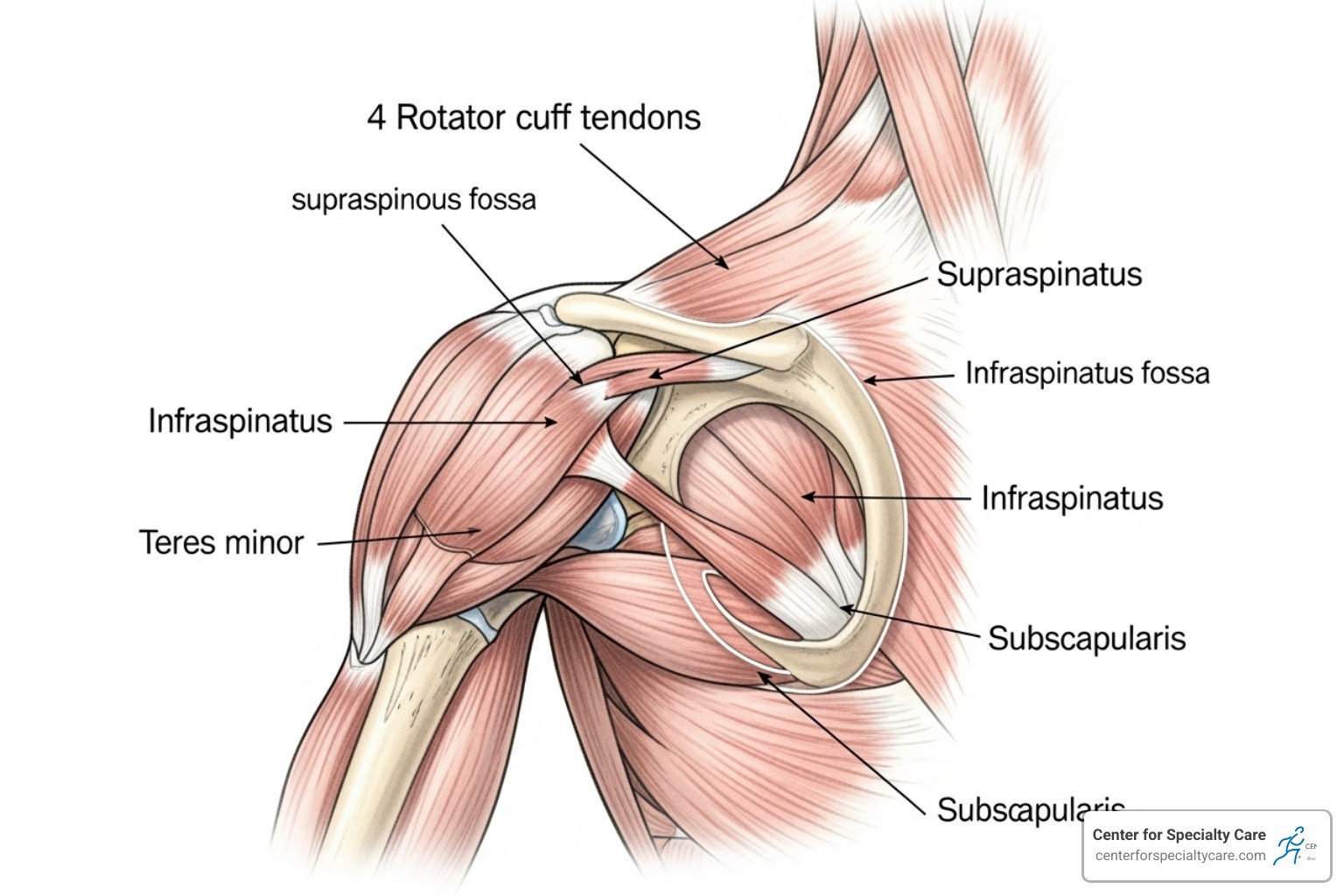
- Rotator cuff muscles and tendons: dynamic stabilizers
These structures work together to keep the arm centered in the socket during movement.
Description of Instability
Subluxation
- Partial slipping of the humeral head out of the socket
Dislocation
- Complete displacement of the humeral head from the socket
When the ligaments, labrum, and capsule are stretched or torn, the shoulder becomes prone to repeated dislocations. This condition is known as chronic shoulder instability.
Causes of Chronic Shoulder Instability
1. Traumatic Dislocation
A sudden injury is the most common cause of the first dislocation.
- Fall on the arm
- Sports injuries
- Accidents
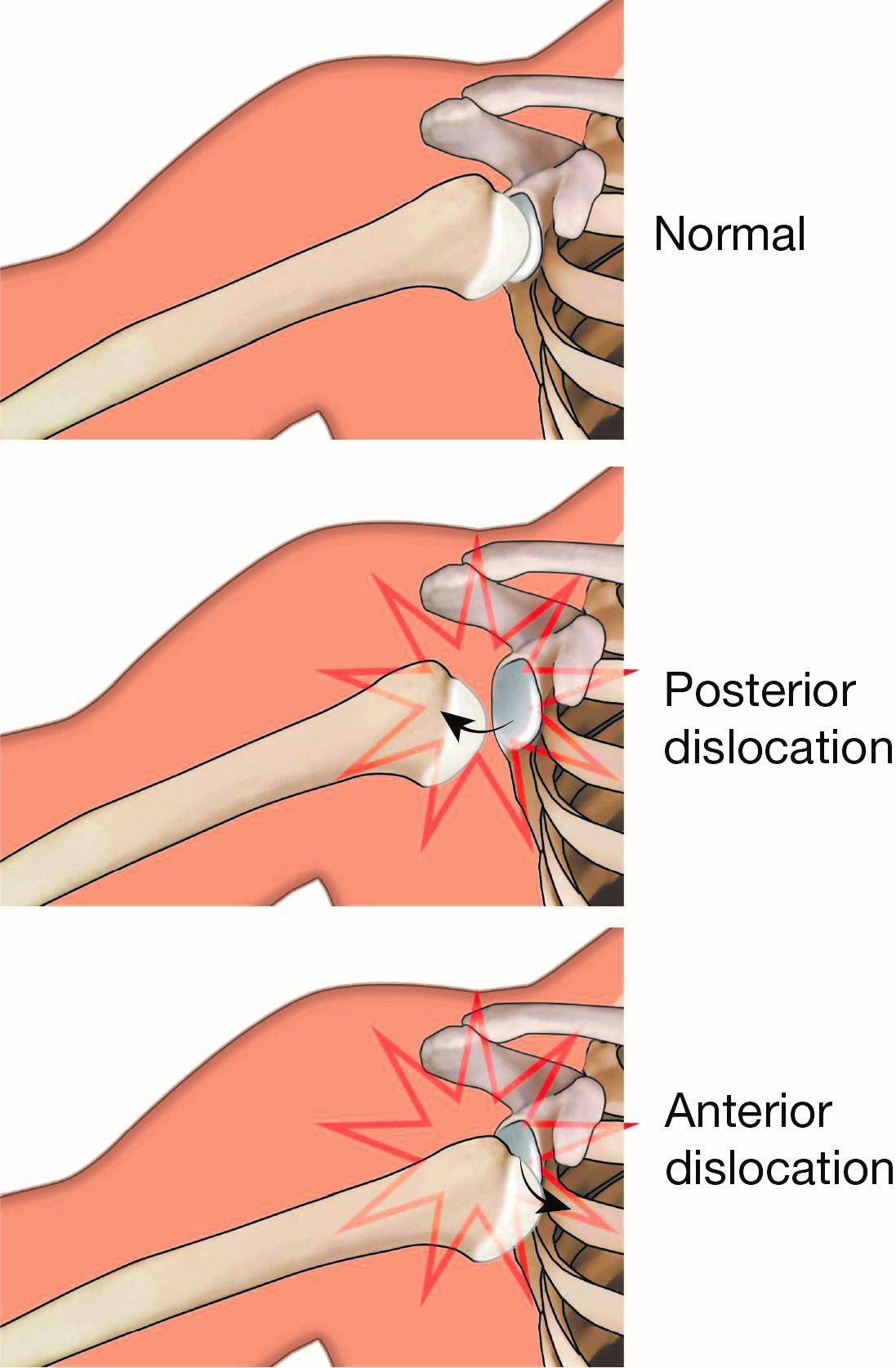
Most dislocations occur toward the front of the shoulder (anterior dislocation).
This may cause:
- Injury to the ligaments
- Tear of the labrum (Bankart lesion)
In some cases, the shoulder may dislocate backward (posterior dislocation).
2. Hyperlaxity (Loose Ligaments)
Some patients develop instability without a major injury.
Causes include:
- Naturally loose ligaments
- Repetitive overhead sports
- Overhead occupational activities
Common in:
- Swimmers
- Tennis players
- Volleyball players
- Overhead laborers
3. Multidirectional Instability
In some patients, the shoulder is unstable in multiple directions:
- Front
- Back
- Downward
These patients often have generalized ligament laxity and may be double-jointed.
Symptoms
Common symptoms include:
- Repeated shoulder dislocations
- Shoulder giving way during activity
- Feeling of looseness or slipping
- Pain after shoulder movement
- Fear of certain arm positions
Evaluation by Dr. Senthilvelan
Clinical Examination
Dr. Senthilvelan performs a detailed evaluation including:
- Instability tests
- Range of motion assessment
- Muscle strength evaluation
- Ligament laxity testing
- Assessment of associated injuries
Imaging Investigations
X-rays
- Detect bone injuries
- Identify dislocation-related changes
MRI Scan
- Shows labral tears
- Detects ligament injuries
- Evaluates rotator cuff
MR Arthrogram
- Dye injected into the joint
- Improves detection of subtle labral injuries
CT Scan
- Used when bone loss is suspected
- Helps plan surgery in recurrent dislocations
Non-Surgical Treatment
Initial treatment is usually conservative.
Treatment Options
- Activity modification
- Anti-inflammatory medications
- Structured physiotherapy
Physiotherapy focuses on:
- Strengthening rotator cuff muscles
- Improving shoulder control
- Enhancing joint stability
Non-surgical treatment is typically continued for several months before deciding on surgery.
Surgical Treatment
Surgery is recommended when:
- Repeated dislocations occur
- Shoulder feels unstable despite therapy
- Imaging shows labral or ligament tears
- Bone loss is present
Dr. Senthilvelan personally performs all stabilization procedures and supervises the full rehabilitation process.
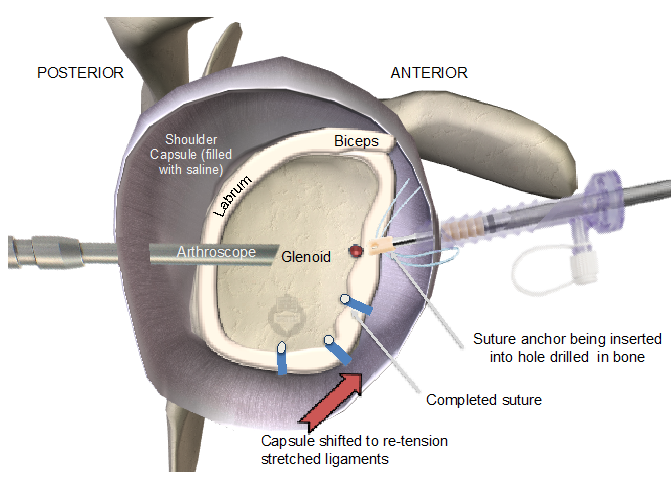
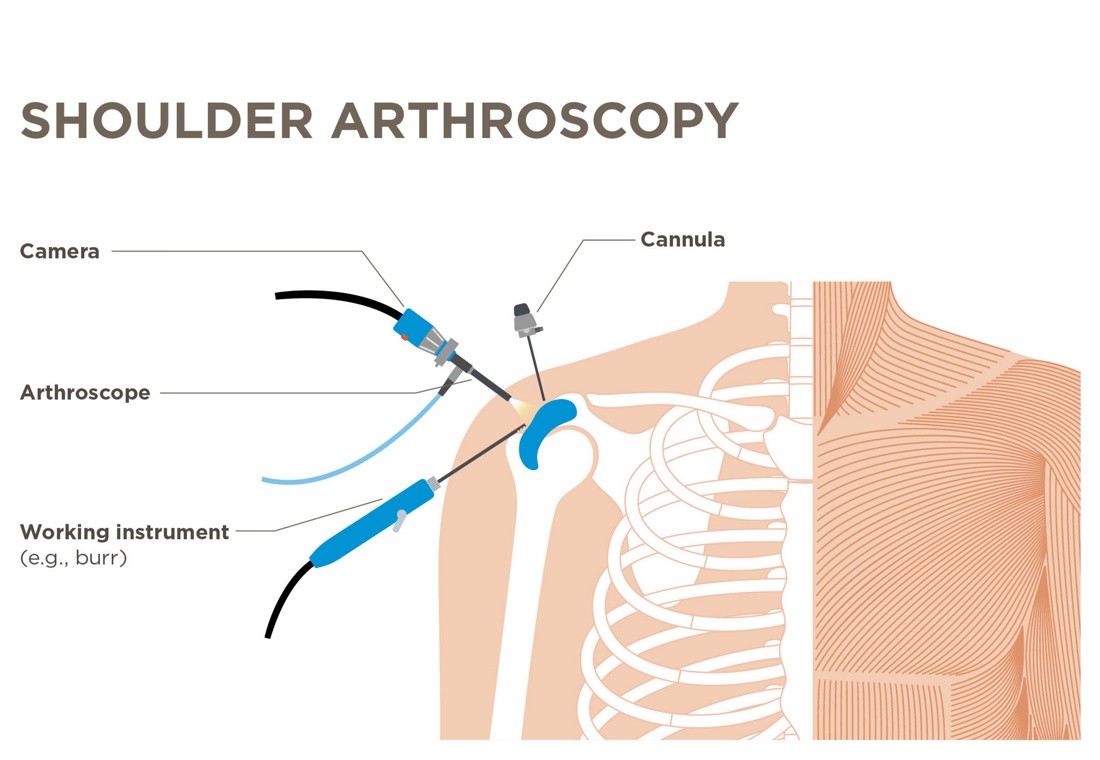
Arthroscopic Stabilization (Bankart Repair)
- Minimally invasive keyhole surgery
- Labrum reattached to the socket using anchors and sutures
- Restores shoulder stability
- Usually performed as a day-care procedure
Bone Procedures (for Severe Instability)
If there is bone loss:
- Bone block procedures may be required
- These restore stability by increasing socket support
Open Stabilization Surgery
- Used in selected cases
- Performed through a small incision
- Provides strong ligament repair
Rehabilitation After Surgery
- Sling immobilization for a few weeks
- Gradual physiotherapy program
- Range of motion exercises first
- Strengthening exercises added later
Dr. Senthilvelan closely monitors recovery and adjusts the rehabilitation plan at each follow-up.
Surgical Outcome
Most patients:
- Regain stable shoulders
- Return to daily activities
- Resume sports after proper rehabilitation
Possible Surgical Risks
Although uncommon, risks include:
- Infection
- Shoulder stiffness
- Recurrent instability
- Nerve injury
Patient FAQs – Chronic Shoulder Instability
Why does my shoulder keep dislocating?
Repeated dislocations usually occur because the ligaments and labrum were damaged during the first injury and did not heal properly.
Can instability heal without surgery?
Some patients improve with physiotherapy, especially if instability is mild. I recommend surgery only when instability persists.
What is a Bankart lesion?
It is a tear of the labrum at the front of the shoulder socket, which commonly causes recurrent dislocations.
How do you diagnose shoulder instability?
Diagnosis is based on clinical examination and imaging such as MRI or CT scans.
When is surgery necessary?
Surgery is recommended if the shoulder continues to dislocate or feels unstable despite proper physiotherapy.
What type of surgery do you perform?
Most patients undergo arthroscopic stabilization, where the torn labrum is repaired using anchors.
Will you perform the surgery yourself?
Yes. I personally perform the surgery and supervise your entire recovery.
How long is recovery after stabilization surgery?
Most patients use a sling for 3–4 weeks and begin strengthening by 6–8 weeks. Full recovery takes about 3–6 months.
Can I return to sports after surgery?
Yes. Most patients return to sports after completing the rehabilitation program.
How often will I be reviewed after surgery?
I schedule regular follow-ups to monitor healing and guide your rehabilitation for the best outcome.

















