Carpal Tunnel Syndrome
Overview & Anatomy
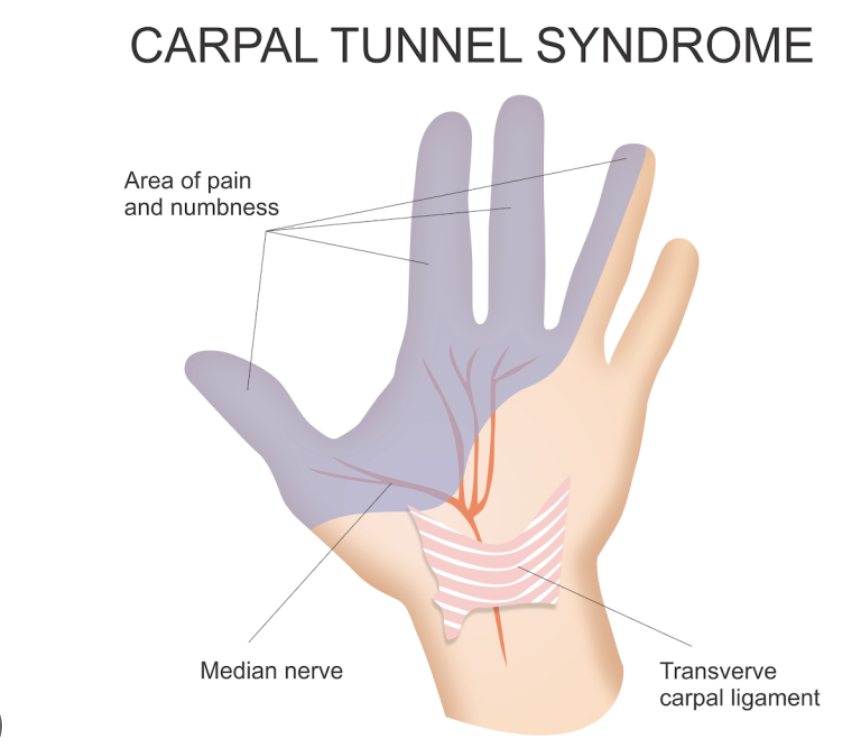
Carpal tunnel syndrome (CTS) is the most common peripheral nerve entrapment condition in the world, affecting approximately 3–6% of the adult population. It results from compression of the median nerve as it passes through the carpal tunnel — a rigid fibro-osseous channel at the base of the palm, bounded by the carpal bones on three sides and the transverse carpal ligament (flexor retinaculum) on the palmar side. The tunnel contains the median nerve and nine flexor tendons (four flexor digitorum superficialis, four flexor digitorum profundus, and flexor pollicis longus). Any process that increases the volume of the tunnel contents or decreases tunnel dimensions can compress the nerve.
Causes & Risk Factors
- Idiopathic: No identifiable cause in the majority — cumulative tenosynovial thickening of the flexor tendons reduces the available space for the median nerve
- Repetitive hand and wrist activity: Sustained gripping, pinching, vibrating tool use, keyboard work with non-neutral wrist posture
- Metabolic and systemic conditions: Diabetes mellitus, hypothyroidism, rheumatoid arthritis, pregnancy (fluid retention), and renal failure on dialysis all significantly increase risk
- Anatomical factors: Square-shaped wrist (wrist ratio index >0.7), congenital variation, wrist fracture malunion, and ganglia within the tunnel
- Pregnancy: Transient CTS due to fluid retention is very common — usually resolves postpartum. Wrist splinting and injection are first-line during pregnancy; surgery rarely required.
- Age and sex: Most common in women aged 45–65
Symptoms
- Numbness and tingling (paraesthesia) in the thumb, index, middle, and radial half of the ring finger — the classic median nerve sensory distribution
- Nocturnal symptoms: Waking at night with burning, tingling, or numbness in the hand is the most characteristic and diagnostically important symptom. Patients typically describe shaking the hand to relieve symptoms (‘flick sign’).
- Symptoms provoked by sustained gripping (driving, reading a newspaper, using a phone), prolonged wrist flexion, and repetitive wrist motion
- Weakness and clumsiness: Thenar muscle wasting (atrophy of the base of the thumb) and weakness of thumb opposition and abduction indicate advanced, prolonged compression
- Whole-hand paraesthesia: Many patients describe diffuse hand numbness that does not respect strict median nerve distribution — this ‘glove’ distribution does not exclude CTS
Diagnosis
Clinical Tests
| Phalen’s Test | Sustained wrist flexion at 90° for 60 seconds reproduces median nerve symptoms — sensitivity 68%, specificity 73% |
| Tinel’s Sign | Percussion over the carpal tunnel at the wrist crease reproduces tingling in the median nerve distribution — sensitivity 50%, specificity 77% |
| Compression Test (Durkan’s) | Direct sustained compression over the carpal tunnel for 30 seconds — the most sensitive clinical test (sensitivity ~87%) |
| Thumb Abduction Strength | Weakness of abductor pollicis brevis (APB) indicates thenar denervation — an advanced sign requiring prompt surgical intervention |
Investigations
- Nerve conduction studies (NCS) and EMG: The gold standard. Confirm the diagnosis, quantify severity (mild, moderate, severe), and identify concurrent proximal compression (cervical radiculopathy, thoracic outlet syndrome — the ‘double crush’ phenomenon). Graded by the Bland classification for surgical decision-making.
- Ultrasound: Cross-sectional area of the median nerve at the level of the pisiform >10–12 mm² is diagnostic. Also identifies compressive lesions (ganglia, lipomata) and guides injections. Increasingly used as an alternative or complement to NCS.
- X-ray: Excludes bony pathology — carpal fracture, arthritis, previous fracture malunion contributing to tunnel narrowing.
Treatment
Non-Surgical (Mild–Moderate CTS)
- Wrist night splint: The single most effective first-line treatment. A neutral-position wrist splint worn at night prevents the sustained wrist flexion that increases carpal tunnel pressure during sleep. Most patients experience significant symptom improvement within 4–6 weeks. Daytime splinting during provocative activities provides additional relief.
- Activity modification: Reducing sustained gripping, avoiding prolonged wrist flexion, and modifying workstation ergonomics
- Corticosteroid injection into the carpal tunnel: Highly effective for short-to-medium-term relief. Provides significant symptom reduction in ~80% of patients at 1 month. Ultrasound-guided injection by Dr. Senthilvelan ensures precise placement around the nerve without intraneural injection. Effects typically last 2–6 months; may be repeated once.
- Oral NSAIDs and diuretics: Limited evidence; may provide modest short-term relief particularly in pregnancy-associated CTS
- Physiotherapy and nerve gliding: Median nerve mobilisation exercises and tendon gliding can reduce intraneural pressure and improve symptom control
When to proceed to surgery: Thenar wasting, permanent numbness (loss of protective sensation), severe NCS changes, or failure of conservative measures after 3–6 months are indications for surgical release. Do not delay surgery in the presence of muscle wasting — motor recovery after established denervation is slow and often incomplete.
Surgical Treatment: Carpal Tunnel Release
Carpal tunnel release (CTR) is one of the most commonly performed and most successful operations in hand surgery. It involves dividing the transverse carpal ligament to decompress the median nerve:
- Open carpal tunnel release: A 3–4 cm incision in the palm allows direct visualisation and complete division of the ligament. The gold standard technique with the lowest recurrence rate. Performed under local anaesthesia as a day-case procedure. Scar tenderness (pillar pain) may persist for 6–12 weeks.
- Endoscopic carpal tunnel release (ECTR): The ligament is divided using a specialised endoscope inserted through a small wrist incision. No palm scar; faster return to grip-intensive work (2–3 weeks vs 4–6 weeks for open). Slightly higher rate of incomplete release. Dr. Senthilvelan will recommend the most appropriate technique for your specific anatomy.
- Recovery: The wound heals within 2 weeks. Finger movement is encouraged from day 1. Grip strength returns to normal at 6–12 weeks. Numbness and tingling typically resolve progressively over 3–6 months. Thenar weakness recovery depends on the duration of denervation before surgery.

Patient FAQs –Carpal Tunnel Syndrome
Will I have full use of my arm after elbow replacement?
For most patients with mild-to-moderate CTS, sensation fully recovers after carpal tunnel release — typically within 3–6 months. Patients with severe or longstanding compression and established thenar wasting may have permanent residual numbness and weakness. This is why early treatment is important — do not wait until your hand is constantly numb or your thumb is wasting.
Can carpal tunnel syndrome come back after surgery?
True recurrence after complete ligament division is rare (<5%). Persistent or recurrent symptoms are more commonly due to incomplete initial release, scar formation (fibrosis around the nerve), or a new compressive lesion. Revision surgery is occasionally required.
I have bilateral carpal tunnel — can both hands be operated at the same time?
Both hands can be operated simultaneously, but this is generally not recommended as it leaves the patient temporarily unable to use either hand independently. Most patients prefer sequential bilateral surgery — the more symptomatic or more severely affected hand first, followed by the other after recovery.
Do I need a general anaesthetic for carpal tunnel surgery?
No. Carpal tunnel release is routinely performed under local anaesthesia (WALANT — Wide Awake Local Anaesthesia No Tourniquet technique) in the outpatient or day-surgery setting. You will be fully awake but comfortable, and can drive yourself home after the local anaesthetic has worn off (usually 2–4 hours).