")
Knee Bursitis (Prepatellar & Pes Anserine Bursitis)
Overview
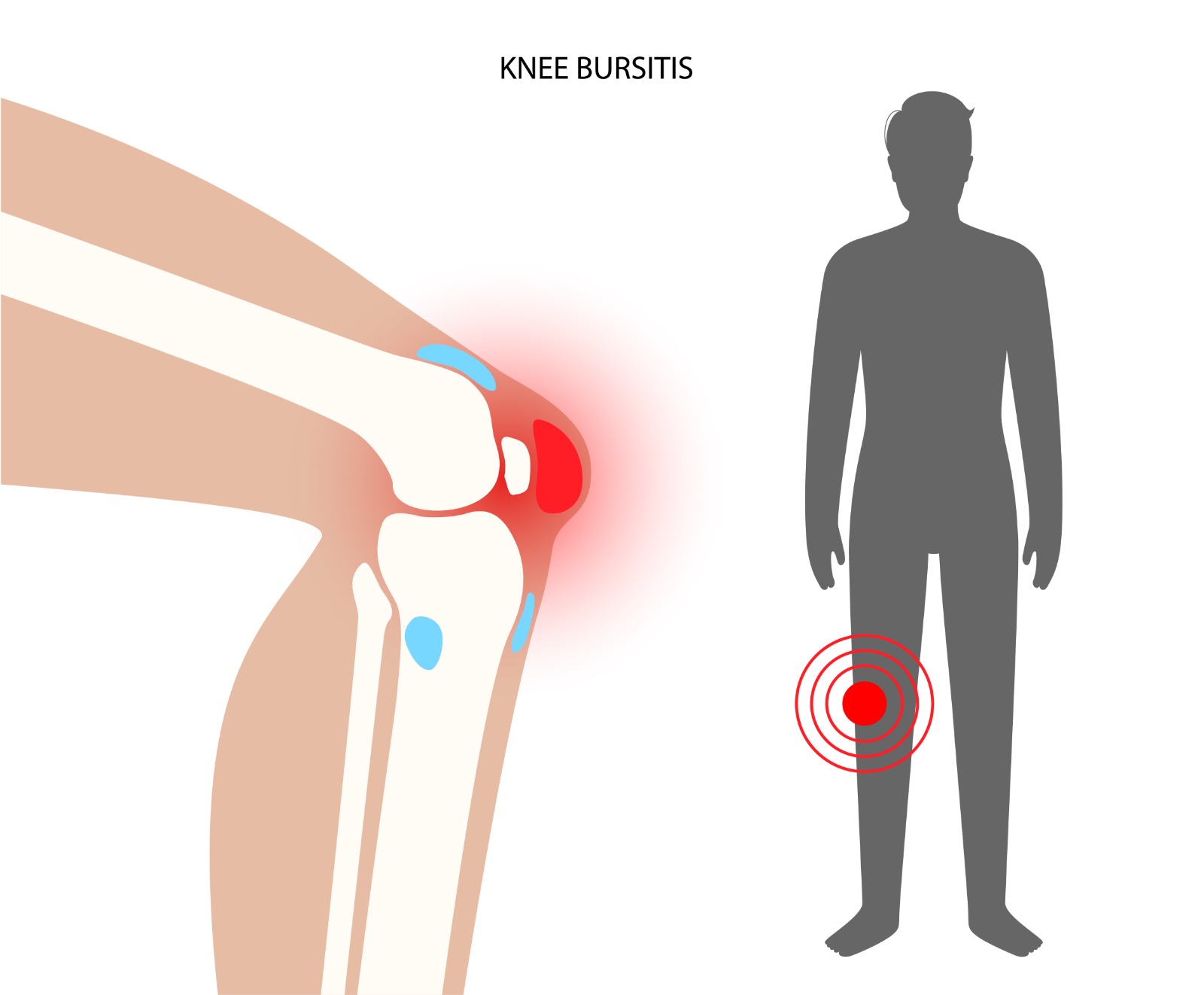
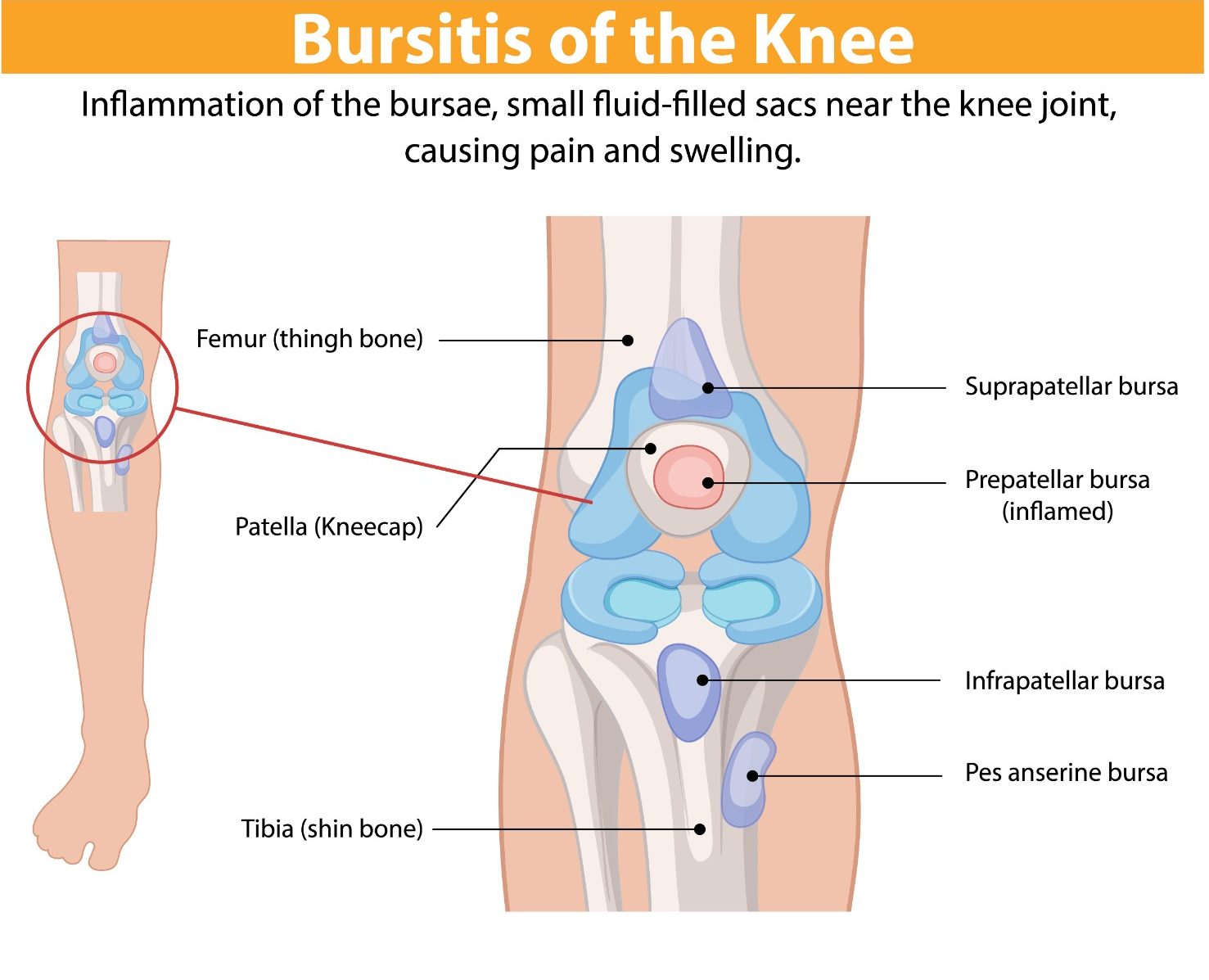
Bursae are small fluid-filled sacs positioned throughout the body at points of friction between tendons, bones, and skin. The knee contains several bursae, the most clinically significant being the prepatellar bursa (over the kneecap), the infrapatellar bursa (below the kneecap), and the pes anserine bursa (at the inner side of the upper tibia). Inflammation of these bursae — bursitis — causes localised pain and swelling. Each bursa has characteristic causes and presentations.
Causes & Risk Factors
- Prepatellar bursitis (‘housemaid’s knee’): Prolonged kneeling — common in carpet layers, plumbers, gardeners, and religious practice involving kneeling
- Direct blow or fall onto the kneecap
- Pes anserine bursitis: Obesity, medial knee osteoarthritis, and tight hamstrings — common in overweight middle-aged and elderly patients
- Septic (infected) bursitis: Bacterial inoculation through skin abrasion or wound over the bursa — a medical emergency requiring urgent drainage
- Gout or pseudogout: Crystal deposition within the bursal sac causing acute inflammatory episodes
Signs & Symptoms
- Prepatellar: Fluctuant (fluid-filled), painless or mildly painful swelling directly over the kneecap — the knee joint itself moves freely
- Pes anserine: Pain and tenderness at the inner side of the knee approximately 2–3 cm below the joint line — often worse at night and on ascending stairs
- Septic bursitis: Rapid onset of warm, red, exquisitely tender bursal swelling, fever, and systemic illness
- Crystal bursitis: Sudden, severe acute inflammation
Diagnosis
Clinical diagnosis based on location and characteristics of swelling. Aspiration of the bursal fluid is essential when infection is suspected — fluid is sent for microscopy, culture, and crystal analysis. MRI or ultrasound delineates the extent of bursitis and any underlying joint pathology.
Treatment Options
- Aseptic prepatellar bursitis: Activity modification, knee padding, aspiration, and corticosteroid injection
- Pes anserine bursitis: Physiotherapy, weight management, corticosteroid injection, and treatment of underlying knee OA
- Septic bursitis: Urgent aspiration, oral or intravenous antibiotics, and surgical bursectomy if failing to resolve
- Surgical excision (bursectomy) for chronic, recurrent, or persistently symptomatic bursae
Patient FAQs – Knee Bursitis (Prepatellar & Pes Anserine Bursitis)
Is knee bursitis serious?
Most forms of aseptic bursitis are not serious and respond well to conservative treatment. However, septic (infected) bursitis is a medical emergency requiring prompt drainage and antibiotics to prevent local tissue destruction and systemic sepsis.
How do I know if my bursa is infected?
Signs of infection include rapid swelling, marked redness and warmth, fever, and systemic illness. Any puncture wound or skin break over the kneecap followed by bursal swelling should be assessed urgently for infection.
Can bursitis come back after treatment?
Recurrence is common if the provocative activity (e.g., prolonged kneeling) continues. Using knee pads, activity modification, and treating underlying conditions (e.g., knee OA in pes anserine bursitis) reduce recurrence risk. Surgical bursectomy provides definitive resolution for recurrent cases.

















