
Quadriceps and Patellar Tendon Rupture
Overview
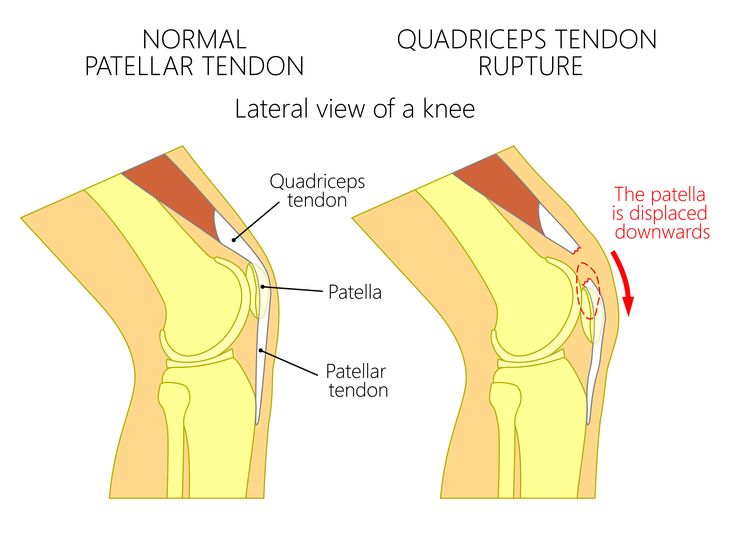
Rupture of the quadriceps or patellar tendon is a serious knee extensor mechanism injury that completely disrupts the ability to straighten (extend) the knee. Quadriceps tendon ruptures occur above the patella, typically in patients over 40, while patellar tendon ruptures occur below the patella and more commonly affect younger, athletic individuals. Both injuries require prompt surgical repair to restore extensor function, and delayed treatment significantly worsens outcomes. Complete ruptures are surgical emergencies.
Causes & Risk Factors
- Sudden forced eccentric quadriceps contraction — landing heavily from a jump or stumbling
- Pre-existing tendon degeneration in older patients — often from chronic tendinopathy, diabetes, gout, or corticosteroid injection
- Systemic conditions weakening tendon tissue: Chronic kidney disease, diabetes mellitus, hyperparathyroidism, lupus
- Previous corticosteroid injection into or near the tendon
- Fluoroquinolone antibiotic use — known to increase tendon vulnerability
Signs & Symptoms
- Sudden, severe pain in the front of the knee at the moment of rupture
- An audible or palpable ‘pop’ or tearing sensation
- Inability to extend the knee or perform a straight leg raise
- Visible gap or defect palpable above (quadriceps) or below (patellar tendon) the kneecap
- Rapid swelling and bruising across the front of the knee
- Patella displaced — riding high (patella alta) in patellar tendon rupture or low (patella baja) in quadriceps rupture
Diagnosis
Clinical diagnosis is straightforward — inability to perform a straight leg raise with an empty arc of extension is pathognomonic. X-rays demonstrate patella alta or baja. MRI confirms the rupture site, extent of tendon damage, and residual continuity.
Treatment Options
- Complete ruptures: Surgical primary repair — reattachment of the tendon through bone tunnels or suture anchors — ideally within 2–3 weeks of injury for optimal outcomes
- Augmentation with a graft for late or re-ruptures where primary tissue is of poor quality
- Post-operative immobilisation in extension followed by progressive physiotherapy
- Return to full sporting activity typically takes 9–12 months
Patient FAQs – Quadriceps and Patellar Tendon Rupture
Can a quadriceps or patellar tendon rupture heal without surgery?
Complete ruptures cannot heal functionally without surgery. The retracted tendon ends cannot bridge the gap spontaneously, leaving permanent extensor mechanism failure. Surgery is essential for complete ruptures.
How important is early surgery for tendon rupture?
Early repair (within 2–3 weeks) is strongly preferable. Tendon ends remain supple and well-approximated. Delayed repair requires grafting to bridge the gap, is technically more challenging, and carries a higher risk of suboptimal outcomes.
What is the expected recovery after tendon repair?
Recovery is a gradual process. Protected weight-bearing begins within weeks of surgery. Active rehabilitation progresses over 3–6 months, with return to sport at approximately 9–12 months, contingent on achieving symmetrical strength and functional confidence.

















