
Patellar Dislocation and Instability
Overview
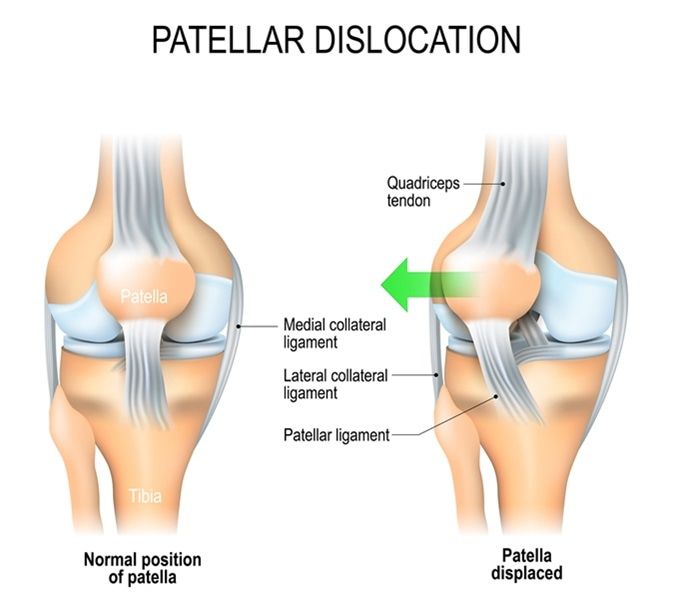
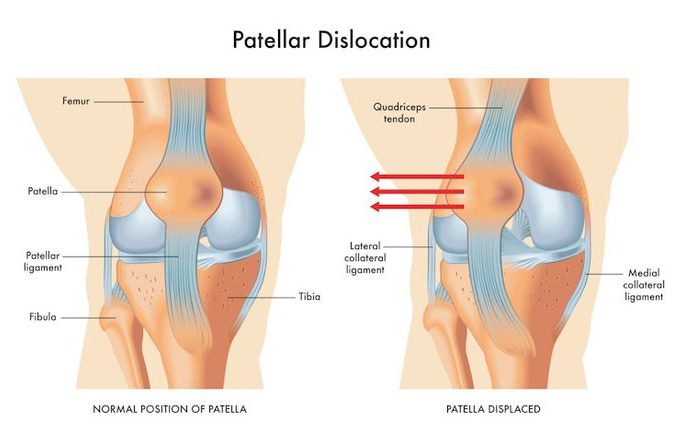
Patellar dislocation occurs when the kneecap (patella) is forcibly displaced from its groove at the front of the femur (the trochlea), typically moving laterally. It is a painful and debilitating injury, most common in adolescent and young adult females, and in individuals with predisposing anatomical risk factors. First-time dislocations carry a significant rate of recurrence — up to 50% in young athletes — and recurrent dislocation leads to progressive damage to the cartilage of the patella and trochlea, contributing to early-onset patellofemoral arthritis.
Causes & Risk Factors
- Sudden twisting of the knee with the foot planted — often during sport
- Direct blow to the patella
- Predisposing anatomical factors: Trochlear dysplasia (a shallow groove), patella alta (high-riding kneecap), increased tibial tuberosity to trochlear groove (TT-TG) distance
- Ligamentous laxity and generalised joint hypermobility
- Weakened medial patellofemoral ligament (MPFL) — the primary soft tissue restraint
Signs & Symptoms
- Acute onset of severe knee pain with visible deformity — the kneecap displaced to the outer side of the knee
- Often spontaneous reduction (kneecap snapping back) as the knee is straightened
- Immediate swelling (haemarthrosis) following dislocation
- Apprehension and reluctance to bend the knee after reduction
- In recurrent instability — a feeling of the kneecap slipping or about to give way
Diagnosis
Clinical examination after reduction, including the patellar apprehension test. X-rays confirm reduction and identify any osteochondral fracture fragments. MRI assesses MPFL integrity, trochlear morphology, cartilage damage, and loose bodies. CT scanning measures TT-TG distance and trochlear dysplasia grade.
Treatment Options
- Acute: Gentle reduction of the dislocated patella (usually spontaneous or in emergency department), immobilisation, and ice
- Non-surgical: VMO strengthening, patellar bracing, and physiotherapy — appropriate for first-time dislocators without significant anatomical risk factors
- Surgical MPFL reconstruction: Reconstruction of the medial patellofemoral ligament — the most common surgical procedure for recurrent instability — restores patellar restraint
- Tibial tuberosity osteotomy (Fulkerson procedure): Bone realignment for patients with elevated TT-TG distance
- Trochleoplasty: Deepening of the trochlear groove for high-grade trochlear dysplasia in selected cases
Patient FAQs – Patellar Dislocation and Instability
Will my knee dislocate again after the first time?
The risk of recurrence depends on age and anatomical risk factors. Young patients (under 25) with predisposing anatomy face recurrence rates of up to 50%. MPFL reconstruction significantly reduces recurrence risk to less than 10% in appropriately selected patients.
Is patellar dislocation the same as kneecap dislocation?
Yes — patellar dislocation and kneecap dislocation refer to the same event: the patella being displaced from its groove on the front of the femur, almost always in the lateral (outward) direction
What is MPFL reconstruction and is it effective?
MPFL reconstruction involves replacing the damaged medial patellofemoral ligament — the primary restraint against lateral patellar displacement — with a graft (usually the patient’s own gracilis or quadriceps tendon). It is highly effective, reducing recurrence rates to under 10% and allowing full return to sport in most patients within 6–9 months.

















