")
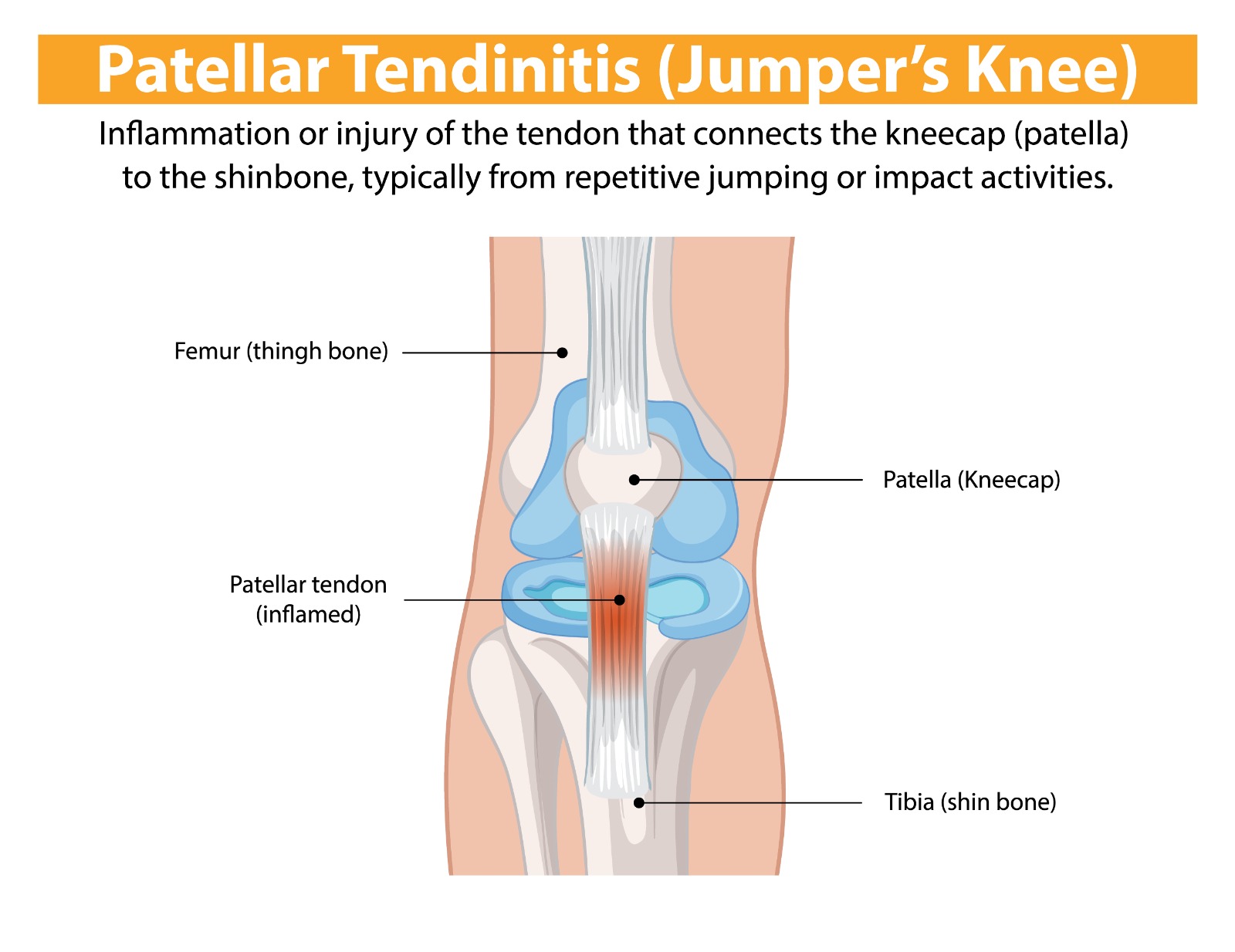
Patellar Tendinopathy (Jumper's Knee)
Overview
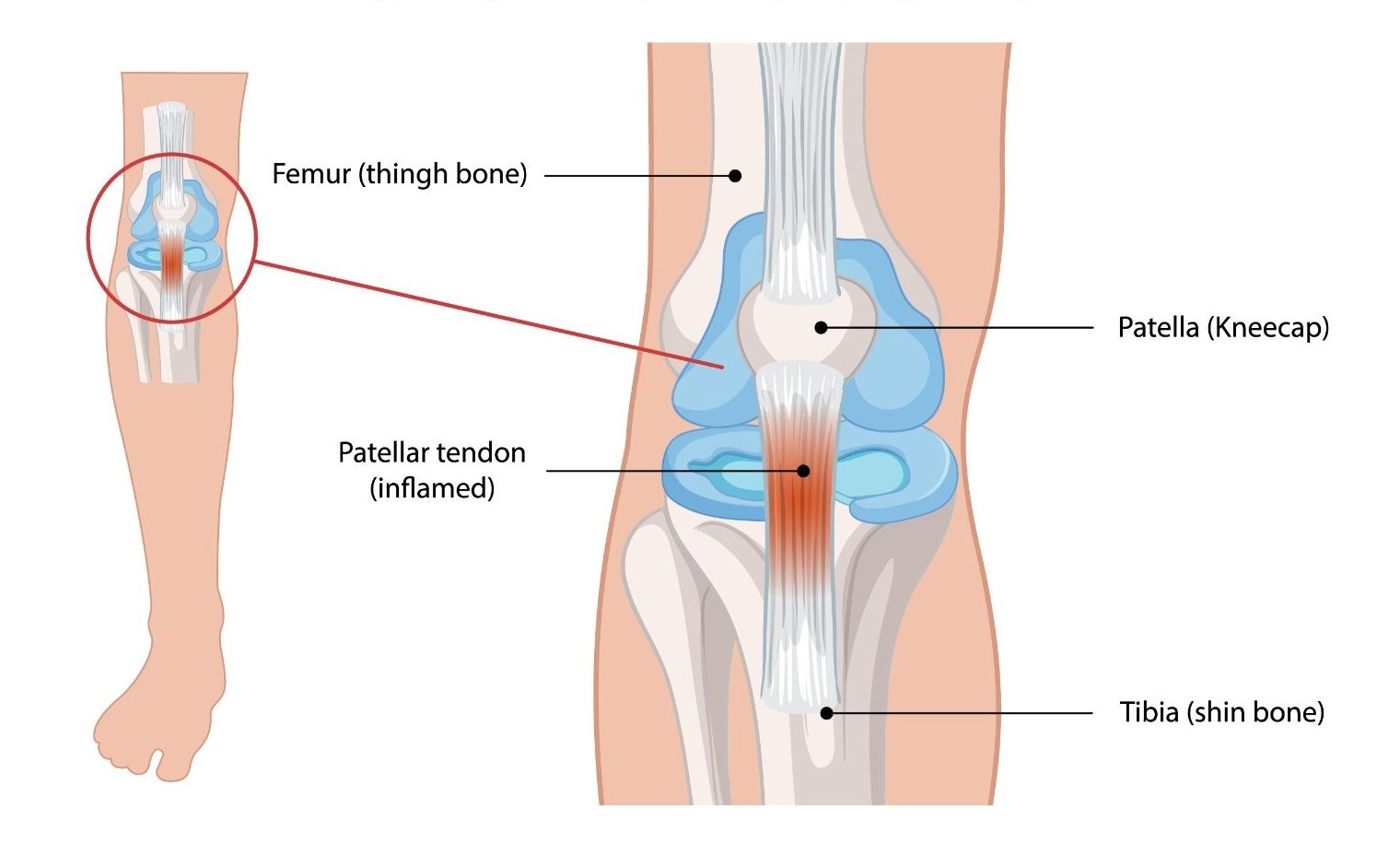
Patellar tendinopathy — commonly known as ‘jumper’s knee’ — is an overuse condition affecting the patellar tendon, which connects the kneecap (patella) to the shinbone (tibia). It is caused by repetitive loading of the tendon beyond its capacity to recover, leading to tendon degeneration, pain, and functional impairment. It is particularly prevalent in jumping athletes — volleyball and basketball players, high jumpers, and footballers — and is one of the most challenging sports injuries to manage due to the tendon’s poor healing response.
Causes & Risk Factors
- Repetitive high-load jumping, sprinting, and explosive quadriceps activity
- Sudden increase in training volume or intensity
- Hard playing surfaces — particularly in indoor sports
- Reduced ankle dorsiflexion, hip flexor tightness, or quadriceps weakness altering patellar tendon loading
- Previous acute tendon injury predisposing to degenerative change
Signs & Symptoms
- Anterior knee pain localised to the inferior pole of the patella (just below the kneecap)
- Pain that is worse with loading the knee — jumping, landing, squatting, and stair descent
- A characteristic ‘warm-up phenomenon’ — stiffness that improves with activity but worsens afterward
- Tenderness on pressing the inferior patellar tendon
- In advanced cases, pain persisting during activity and progressively limiting sport participation
Diagnosis
Clinical assessment using the VISA-P questionnaire quantifies severity and monitors progress. Ultrasound demonstrates tendon thickening, neovascularisation, and hypoechoic areas of degeneration. MRI provides detailed assessment for surgical planning or when diagnosis is uncertain.
Treatment Options
- Load management: Structured reduction in provocative activity combined with targeted rehabilitation
- Progressive tendon loading programme (isometric, isotonic, heavy slow resistance) — the cornerstone of treatment
- Shockwave therapy: Extracorporeal shock wave therapy (ESWT) — an effective adjunct for chronic cases
- Platelet-rich plasma (PRP) injection: Promotes tendon healing in chronic, refractory tendinopathy
- Surgical: Arthroscopic or open excision of degenerative tendon tissue for cases unresponsive to 6+ months of conservative treatment
- Sport-specific return-to-play programme with load monitoring
Patient FAQs – Patellar Tendinopathy (Jumper's Knee)
Is jumper's knee serious?
Patellar tendinopathy can become a chronic, career-limiting condition if not managed correctly. Early diagnosis and structured rehabilitation optimise outcomes. Ignoring symptoms and continuing to load the tendon aggressively accelerates degeneration and risks complete tendon rupture.
How long does patellar tendinopathy take to heal?
Recovery time varies considerably — mild cases may improve within 3–6 months of structured rehabilitation. Chronic, degenerate tendinopathy may require 12–18 months of progressive loading and adjunct treatments before return to full sport.
Are steroid injections useful for jumper's knee?
Corticosteroid injections are generally not recommended for patellar tendinopathy. Evidence suggests they may provide short-term pain relief but can weaken tendon tissue and increase long-term rupture risk. PRP injections are a preferable biological treatment option.

















