")
Meniscus Tear
Overview
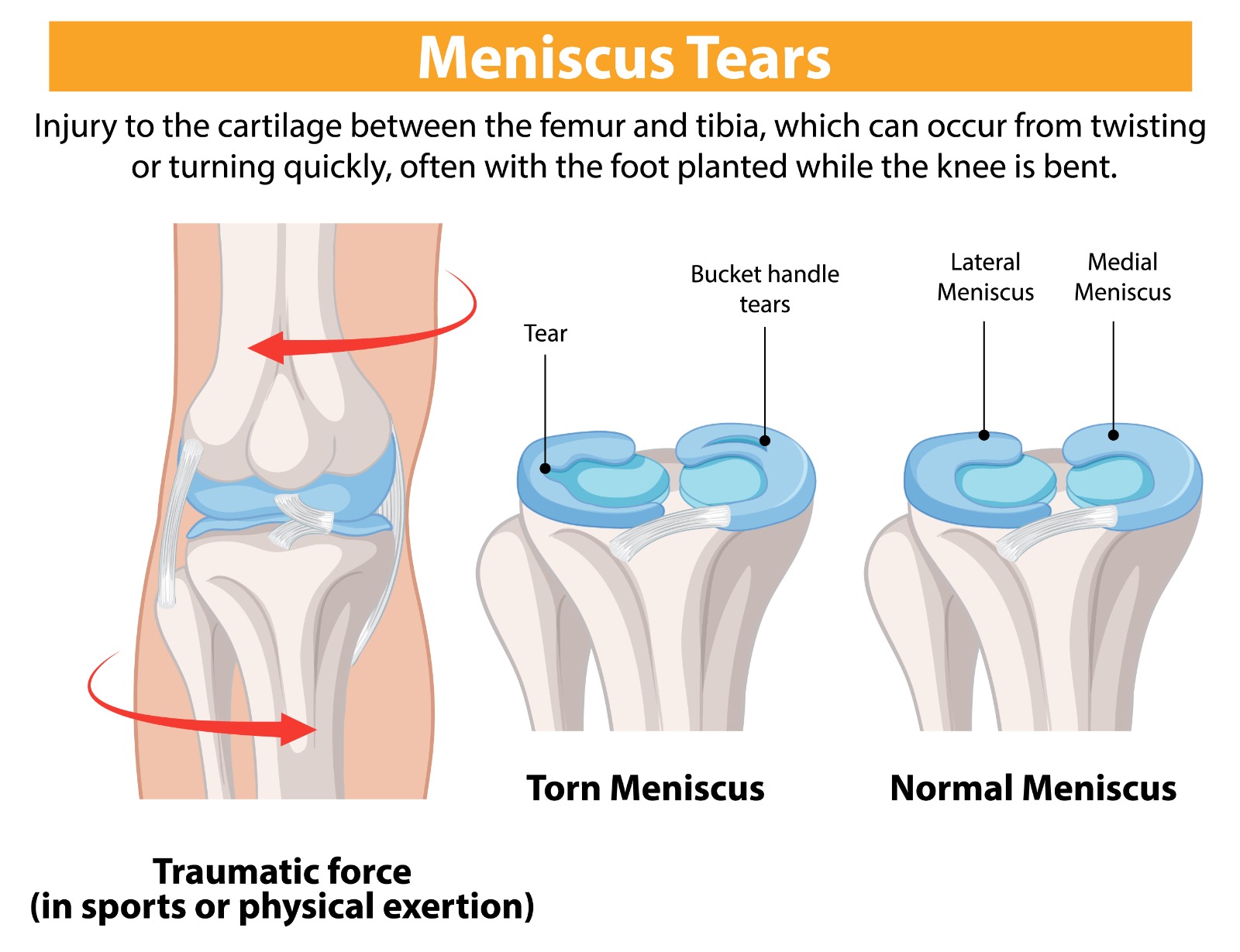
The menisci are two C-shaped fibrocartilaginous discs — the medial and lateral meniscus — that sit between the femur (thigh bone) and tibia (shin bone) within the knee joint. They act as shock absorbers, load distributors, and stabilisers of the knee. Meniscal tears are among the most frequent knee injuries in both athletes and the general population. Tears may result from acute twisting injuries during sport or from degenerative wear in older adults, and they vary considerably in size, shape, and clinical significance.
Causes & Risk Factors
- Acute twisting or pivoting of the knee during sport — often concurrent with ACL injuries
- Deep squatting or kneeling, particularly with the knee under load
- Age-related degenerative thinning of meniscal tissue — even minor activity may cause tearing
- Repetitive microtrauma in occupations or sports requiring squatting
- Associated with knee malalignment (varus or valgus) and ligamentous instability
Signs & Symptoms
- Pain at the inner (medial) or outer (lateral) joint line of the knee
- Swelling developing over hours to days after injury
- Clicking, locking, or catching sensation within the knee joint
- Inability to fully straighten the knee (locked knee) with bucket-handle tear
- Pain with squatting, pivoting, or ascending and descending stairs
- Joint line tenderness on clinical examination
Diagnosis
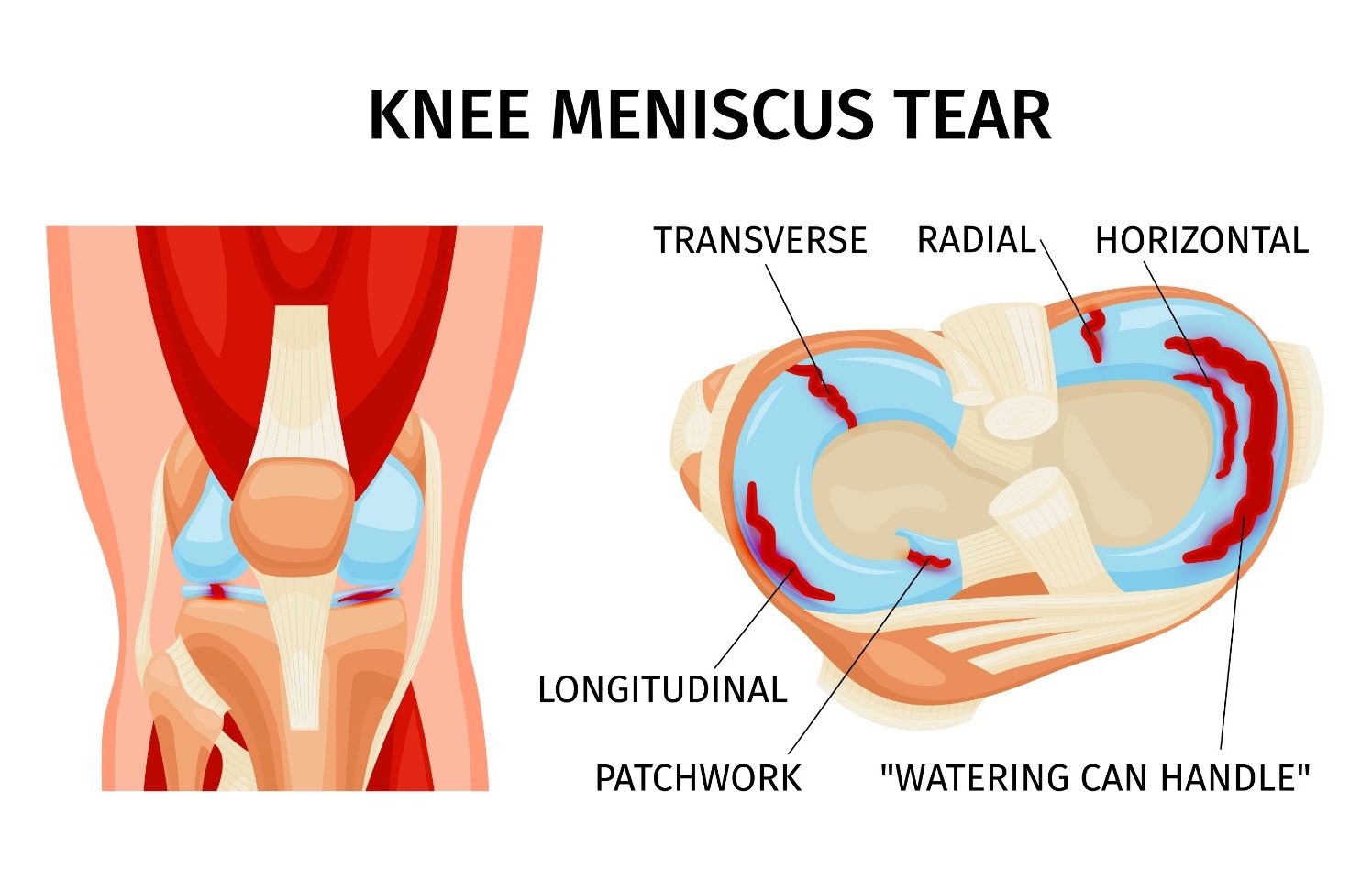
McMurray’s test and Thessaly’s test elicit characteristic joint-line pain and clicking during examination. MRI is the standard diagnostic investigation, accurately identifying tear size, location, pattern (horizontal, radial, bucket-handle, root tears), and vascularity of the affected zone — all crucial for treatment planning.
Treatment Options
- Non-surgical: Physiotherapy, activity modification, and anti-inflammatory medication for minor, stable, degenerative tears in older patients
- Corticosteroid or hyaluronic acid injection for symptom management in degenerative tears
- Arthroscopic partial meniscectomy: Removal of the torn, unstable fragment — most common surgical procedure, rapid recovery
- Arthroscopic meniscal repair: Suturing of peripheral (vascular zone) tears — particularly in young patients — to preserve meniscal tissue and reduce long-term arthritis risk
- Meniscal transplantation for young patients following total meniscectomy
Patient FAQs – Meniscus Tear
Will my meniscus tear heal without surgery?
Small, peripheral tears in the vascular zone of young patients can sometimes heal with conservative management. However, symptomatic tears causing locking, persistent pain, or mechanical symptoms generally require arthroscopic surgery.
Is it better to repair or remove the torn meniscus?
Preserving the meniscus through repair is always preferable when technically feasible. Studies confirm that meniscal loss leads to earlier onset of knee arthritis. Repair is recommended for young patients with peripheral, acute tears. Partial meniscectomy is appropriate for complex or degenerative tears not amenable to repair.
How long does recovery take after meniscus surgery?
Partial meniscectomy allows return to normal activities within 4–6 weeks and return to sport within 6–8 weeks. Meniscal repair requires 3–4 months of protected rehabilitation due to the healing time required, with return to pivoting sport at 4–6 months.

















