")
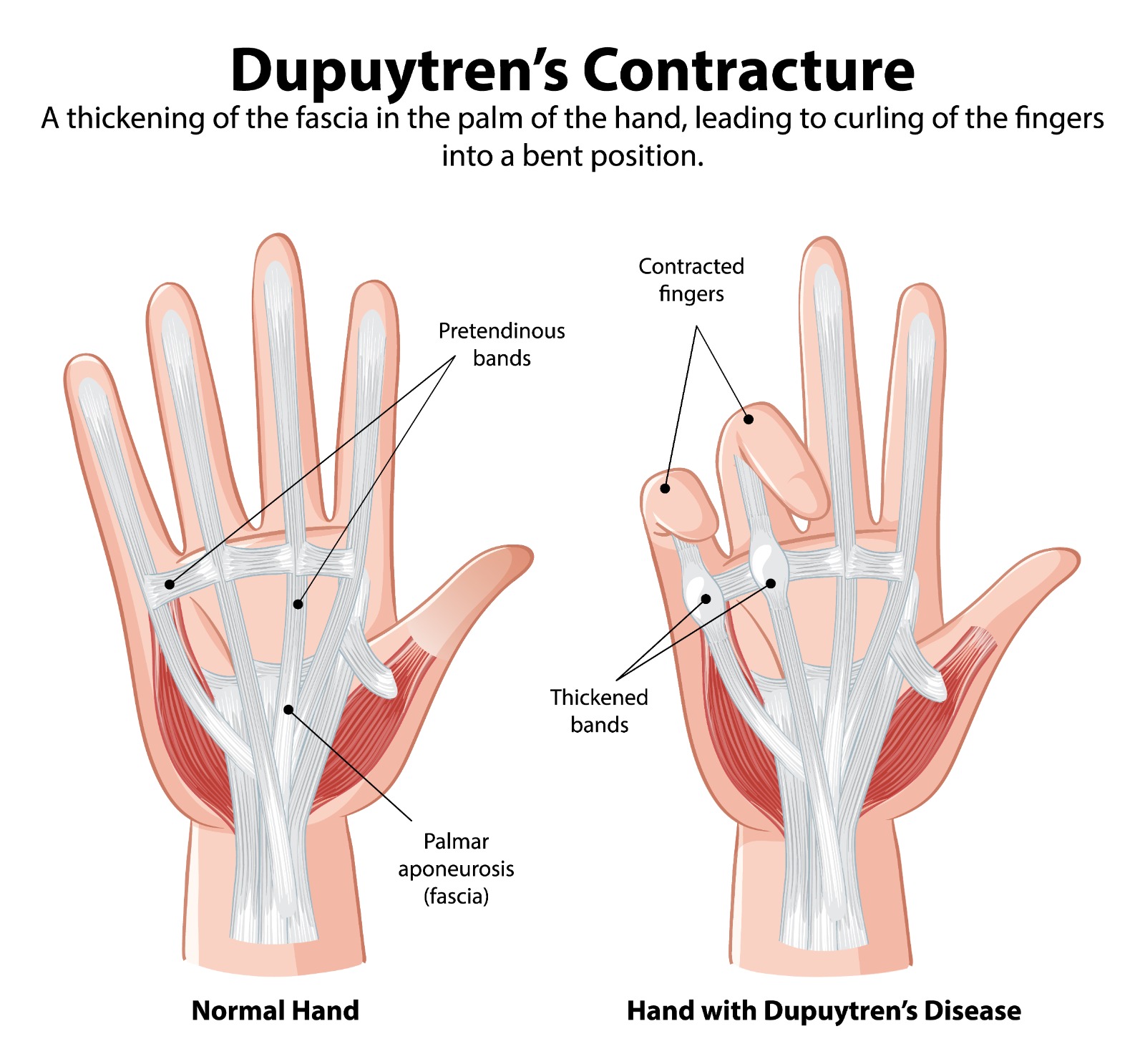
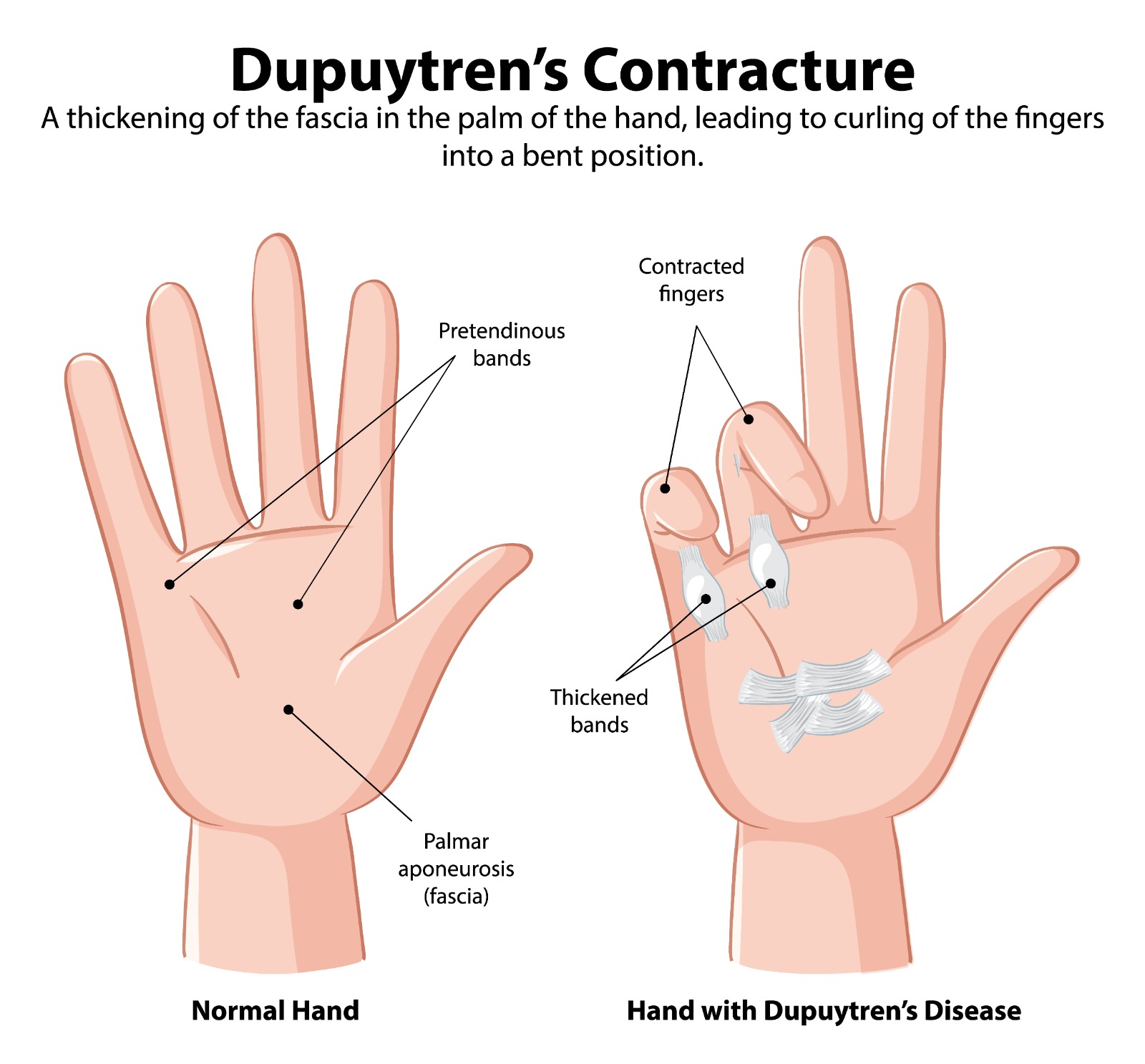
Dupuytren's Contracture
Overview
Dupuytren’s contracture is a progressive fibroproliferative disorder of the palmar fascia — the fibrous tissue layer beneath the skin of the palm — in which abnormal myofibroblast activity leads to the formation of nodules and cords of dense collagen. As these cords mature and contract, they tether the overlying skin and draw the fingers (most commonly the ring and little fingers) into progressive flexion contracture, ultimately preventing full finger extension.
The condition is strongly associated with Northern European ancestry (‘Viking disease’) and is familial in approximately 70% of cases. It is part of the Dupuytren’s diathesis — a systemic fibroproliferative tendency that includes Ledderhose disease (plantar fascia), Peyronie’s disease (penile fascia), and knuckle pads (Garrod’s pads on the dorsal PIP joints).
Risk Factors
- Genetics: The most important factor — strong family history in Northern European descent
- Diabetes mellitus: Up to 3× increased risk; tends to produce bilateral, more indolent disease
- Epilepsy and anti-epileptic medications (particularly phenobarbitone)
- Alcohol excess and liver disease
- Smoking: Implicated in some studies via microvascular effects
- Age and sex: Most common in men over 50; male-to-female ratio approximately 6–7:1
Symptoms & Progression
- Early stage: Painless nodule(s) in the palm — most commonly in the distal palm in line with the ring finger. Pitting or puckering of the overlying skin may be present. No functional deficit.
- Progressive stage: A cord develops proximal to the MCP joint, extending into the finger. Progressive MCP and PIP joint contracture develops over months to years.
- Advanced stage: Fixed flexion of the MCP and PIP joints — the hand cannot be placed flat on a table (positive ‘tabletop test’). Severe functional impairment: difficulty with handshakes, wearing gloves, putting hands in pockets, and using machinery.
Treatment
Observation
Early disease with no functional deficit requires no intervention — observation with annual review. Patients should be counselled on warning signs of progression.
Needle Fasciotomy (Percutaneous Needle Aponeurotomy — PNA)
A needle is inserted through the skin at multiple points along the Dupuytren’s cord and used to perforate and weaken the cord, which is then ruptured by forced finger extension. Performed under local anaesthesia in clinic. Advantages: minimal recovery, can be repeated. Disadvantages: higher recurrence rate than surgery (50% recurrence at 5 years). Best suited to cord-only disease (MCP contracture) in elderly patients or those unwilling or unable to undergo surgery.
Collagenase Clostridium Histolyticum Injection (Xiapex)
Injectable collagenase enzyme is injected directly into the Dupuytren’s cord — the enzyme digests the collagen of the cord. 24 hours later, the cord is ruptured by forced extension under local anaesthesia (manipulation procedure). Effective for single-cord, single-joint MCP contractures. Recurrence rates similar to needle fasciotomy at 3–5 years.
Surgical Fasciectomy
- Segmental fasciectomy: Multiple segments of the cord are excised without complete dissection — lower complication rate, faster recovery, but higher recurrence risk
- Regional fasciectomy (selective): The involved cord and immediately adjacent tissue are excised under direct visualisation. The gold standard surgical technique — lowest recurrence rate, most complete correction. Performed under regional anaesthesia (axillary block or Bier’s block) or WALANT.
- Dermofasciectomy: Excision of cord, fascia, and overlying skin with skin graft replacement — used for recurrent disease or when involved skin cannot be preserved. Lowest recurrence rate of any technique (skin graft appears resistant to Dupuytren’s recurrence).
- Recovery: Wound healing 2–3 weeks; physiotherapy with extension splinting for 3–6 months post-operatively to maintain correction and prevent scar contracture; full recovery 6–12 weeks.
PIP joint contracture: MCP joint contractures correct reliably with all treatment modalities. PIP joint contractures (flexion of the middle finger joint) are more resistant — complete correction is less reliable, particularly for contractures >60°. PIP contractures >30° should be treated early for the best outcome.
Patient FAQs –Dupuytren's Contracture
Will Dupuytren's disease affect all my fingers?
Not necessarily. Disease severity and progression vary considerably. Some patients develop a single cord affecting one finger that remains stable for decades; others develop progressive bilateral, multifinger involvement. The diathesis factors (early onset, bilateral disease, ectopic disease, family history) predict a more aggressive course.
Will the contracture come back after treatment?
Recurrence is a characteristic feature of Dupuytren’s disease regardless of treatment modality. Rates at 5 years: fasciectomy ~25–40%; needle fasciotomy and collagenase ~50%. Recurrence can be retreated. The goal is not to cure but to restore and maintain function over the patient’s lifetime.
Is Dupuytren's disease painful?
Early nodules can be tender and uncomfortable, but established cords and contractures are typically painless. Pain is not a primary feature of Dupuytren’s. If your Dupuytren’s disease is painful, Dr. Senthilvelan will assess whether there is a concurrent condition (carpal tunnel syndrome, trigger finger, and arthritis all co-exist with increased frequency in Dupuytren’s patients) contributing to the discomfort.