De Quervain's Tenosynovitis
Overview
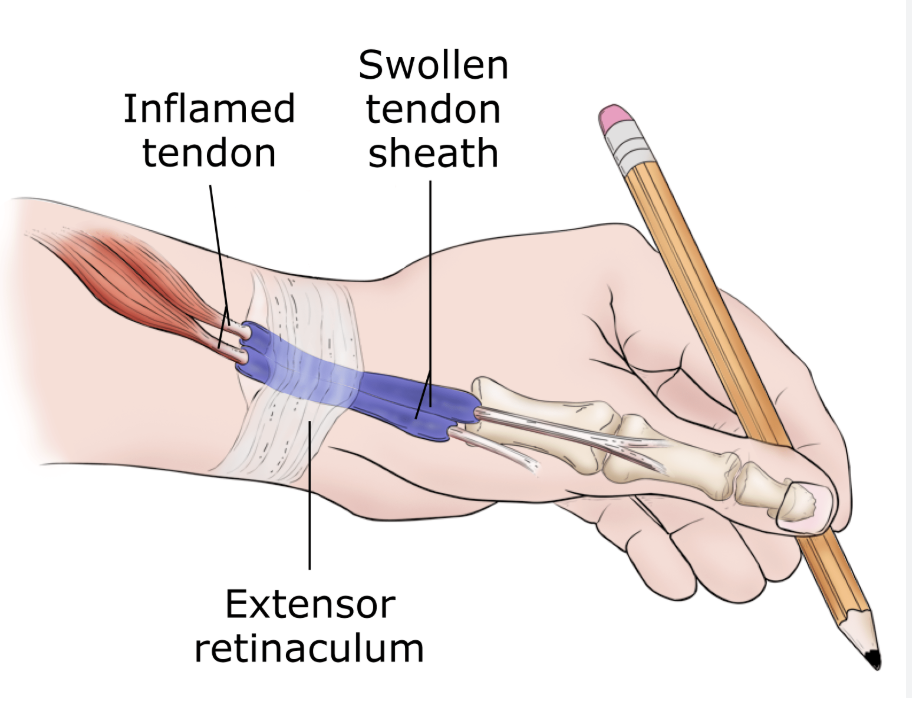
De Quervain’s tenosynovitis is a stenosing tenosynovitis affecting the first dorsal compartment of the wrist — the fibro-osseous tunnel through which the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons pass around the radial styloid process. When the synovial lining of this tunnel becomes thickened and inflamed, the tendons can no longer glide smoothly, producing pain, swelling, and restricted thumb movement. It is one of the most common causes of radial-sided wrist and thumb pain.
Causes & Risk Factors
- New mothers and caregivers: The condition is strongly associated with the repetitive lifting and pinching required when caring for a newborn infant — holding the baby with the thumbs abducted and wrists radially deviated. Postpartum hormonal changes may also contribute to tendon sheath swelling.
- Repetitive thumb and wrist activities: Racket sports, golf, gardening, texting, and occupational activities involving sustained pinch grip
- Age 30–50; approximately 8–10 times more common in women than men
- Anatomical variant: A septum dividing the first compartment into two sub-tunnels (present in ~50–75% of patients) significantly increases surgical failure rate if not identified and released
Symptoms
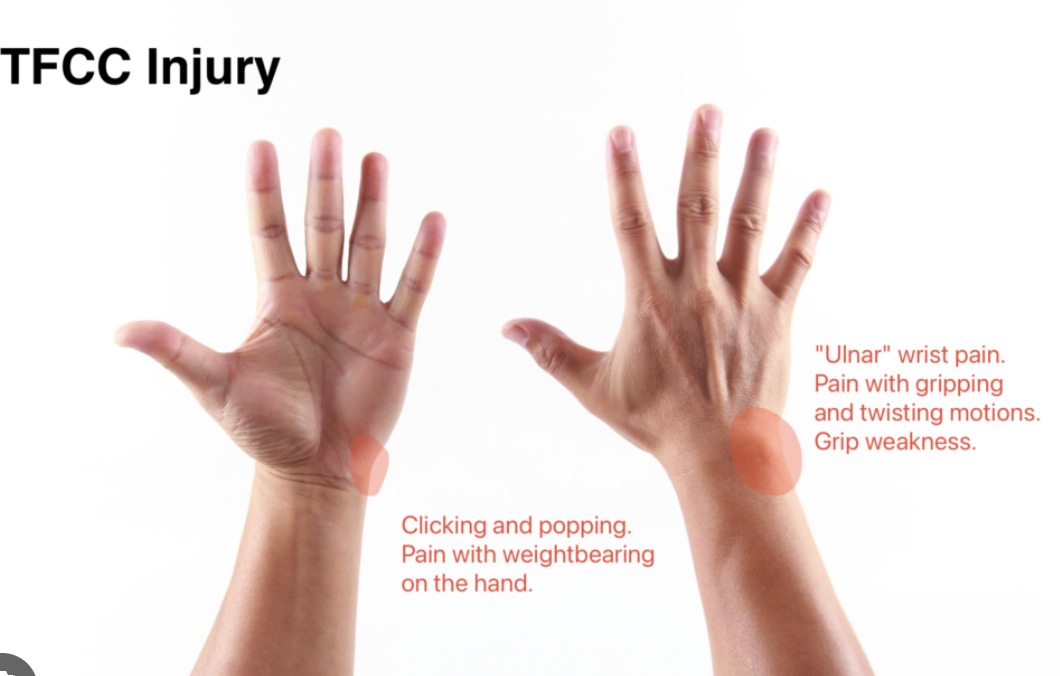
- Radial-sided wrist and thumb pain: Localised to the radial styloid and first compartment, radiating proximally into the forearm and distally into the thumb
- Swelling and tenderness directly over the first dorsal compartment at the radial styloid
- Pain with pinching, gripping, lifting (particularly with the thumb extended), and picking up objects
- A catching or triggering sensation as the thickened tendons attempt to glide through the narrowed tunnel
Finkelstein's Test
The most sensitive and specific clinical test for de Quervain’s: the thumb is flexed into the palm and grasped by the fingers, and the wrist is then deviated in the ulnar direction. Sharp pain reproduced at the radial styloid is a positive result. Note: This test is frequently painful in normal individuals — the pain must be at the first compartment and must reproduce the patient’s typical symptoms.
Treatment
Non-Surgical
- Thumb spica splint: Immobilises the wrist and thumb in a functional position, resting the inflamed tendons. Worn for 4–6 weeks, full-time initially then weaned as symptoms improve. Particularly effective in mild-to-moderate cases.
- Corticosteroid injection into the first dorsal compartment: The most effective non-surgical treatment. A single injection into the tendon sheath (not the tendon itself) provides complete relief in approximately 60–70% of cases. Success rate lower if a septum is present. A second injection may be offered if partial improvement was achieved.
- Activity modification: Avoiding provocative thumb and wrist activities during the treatment period
- Physiotherapy: Tendon gliding exercises, postural retraining, and ergonomic modification
Surgical Release
Surgery is offered when conservative treatment has failed after 3–6 months, or when symptoms recur repeatedly:
- First dorsal compartment release: Performed under local anaesthesia as a day-case procedure. A small incision over the first compartment allows direct visualisation and complete release of the retinaculum. Critical step: identification and release of any internal septum to prevent incomplete decompression. The radial sensory nerve must be carefully protected throughout.
- Recovery: Light hand use within days; return to full activity within 2–4 weeks. Scar maturation takes 3–6 months.

Patient FAQs –Carpal Tunnel Syndrome
I had a baby 3 months ago and my wrist is very painful — is this de Quervain's?
Almost certainly. New-onset radial wrist pain in a new mother is de Quervain’s tenosynovitis until proven otherwise. A clinical assessment with Finkelstein’s test will confirm. The good news is that most cases respond well to a corticosteroid injection and splinting, and many resolve spontaneously as baby-holding patterns change. Please contact Dr. Senthilvelan’s clinic for an early assessment.
Will the injection hurt?
A fine needle injection into the tendon sheath is mildly uncomfortable but well tolerated. Dr. Senthilvelan uses a small amount of local anaesthetic in the injection mixture to reduce discomfort. Most patients describe the injection as significantly less painful than their condition