")
Recurrent dislocation of Shoulder
MBBS, MRCS(UK) FRCS (Tr &Ortho), FEBOT(France), Fellow European Board Orthopaedics and Trauma., D Ortho,Dip SICOT(Honk Kong).
What is its cause?
A ring of cartilage surrounds the shallow socket of the shoulder joint (glenoid). This ring is called the labrum. The glenoid labrum increases the depth of the socket making the shoulder joint more stable. A tough, but thin elastic tissue (capsule) further surrounds the shoulder like a bag. The capsule contains a series of ligaments or bands, which connect the humerus to the glenoid.
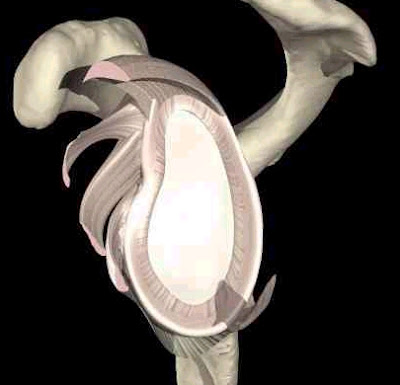
Labrum deepens the glenoid to provide more stability.
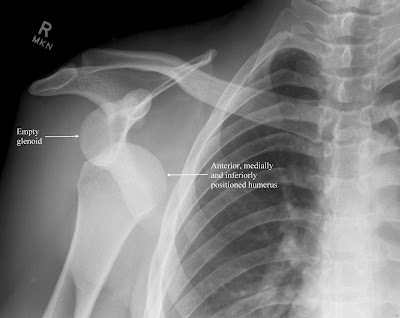
X rays showing dislocation of shoulder joint
The force that causes this injury can cause the labrum to be torn from the socket making it shallow. This lesion is known as a Bankart’s lesion and it can lead to further episodes of subluxation or dislocation. Sometimes a relatively minor force may dislocate the shoulder for the first time and the patient may feel a pop as it reduces by itself. This will occur in people who have normal but lax joints. This is referred to as an atraumatic dislocation.
The symptoms of shoulder instability will range from obvious repeated dislocations, to just pain with certain activities or shoulder positions. Patients may complain of clicking or popping of the shoulder, the arm suddenly ‘feeling dead’ or the shoulder been generally weak.
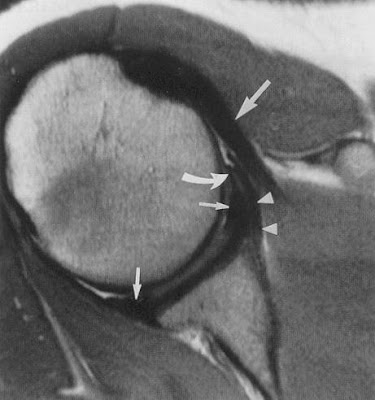
MRI Scan of shoulder showing labral injury
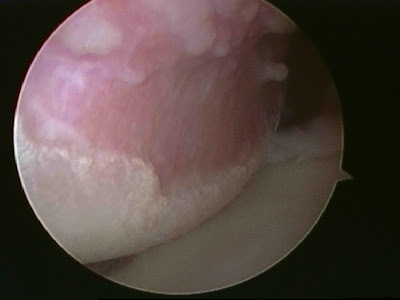
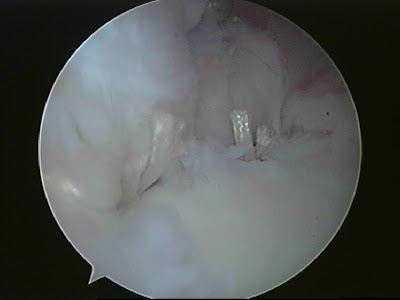
Arthroscopic picture showing Hill Sachs lesion
3. Physiotherapy is the initial line of management in patients who have developed atraumatic type shoulder instability, due to muscle imbalance or abnormal patterns of muscle activity. Some of these cases may not respond to physiotherapy and may need surgical intervention.

Picture above showing Labral detachment
Picture showing completed Arthroscopic(key hole) repair.
Open surgery for bony defects: If there is a significant bone loss, keyhole surgery is not advised. In such circumstances an open operation (Laterjet Procedure) is performed. This procedure involves transfer of a small bone (tip of corocoid process) with its muscle attachments, to the front of the shoulder socket. The transferred bone is fixed with 1or 2 screws.
If the above conditions are not treated it is likely that the symptoms will persist. It may be that the shoulder will become less troublesome if activities that cause the problems are stopped. It is possible that an unstable shoulder may cause arthritis in the long term but there are no convincing long term studies that conclude this.
Surgical treatment for traumatic shoulder instability, when the shoulder repeatedly dislocates forward, has a more than 90% success rate.
2. Loss of movement is possible especially after open surgery.
3. Damage to the nerve or blood vessels is possible.
4. The operation may fail in about 5-8 % of the patients.
5. If the repair is too tight, osteoarthritis of the shoulder may result in the long term.
7. Any surgical intervention has the risk of developing complications that are unpredicted. These complications may have the potential to leave the patient worse than before surgery.

















